
INTRODUCTION
The concept of graduate capability has become somewhat recognised in the higher education sector and, more recently, in nursing practice and education (Hanks et al., 2021). Capability is not limited to one dimension; it is a comprehensive concept involving multiple dimensions in nursing, including clinical judgement capability, interprofessional capability, and clinical reasoning capability (Bromley, 2015). Further, capability has been noted to include a wide range of abilities and characteristics, including knowledge, skills, and personal qualities (Bromley, 2019) and is seen as essential to patient safety and the quality of care provided (Torabizadeh et al., 2019). Capability in nursing practice accommodates the intricacy and complexity of nursing as it evolves and changes in not only predictable specialist contexts but also in unexpected and unstable circumstances (Torabizadeh et al., 2019). Overall, capability is demonstrated through having the ability to work and problem-solve in familiar and unfamiliar contexts having appropriate knowledge and reasoning skills, justified confidence in clinical decision-making, the ability to learn from success and failures, and being able to demonstrate professionalism in a holistic approach to practice (Fergusson et al., 2020; Torabizadeh et al., 2019). This combination of capabilities is at the core of nursing practice, where nurses can take action in uncertainty to learn how to do better, signalling where new graduate capability development may be elucidated.
To date, no standardised approach to evaluating nurse capabilities exists. Surveys are commonplace, however, these are limited to broader contextual capabilities and are usually provided from a singular, self-report perspective. Research in the field rarely provides insights into what new graduate nurse capabilities look like in practice. This study aims to identify how new graduate nurses’ capabilities are observed in practice and whether they differed between two groups of new graduates completing a new graduate programme, one inclusive of a postgraduate course and the other not.
The evidence around the impact of completing postgraduate education on capabilities is largely quantitative and survey-based and qualitative methods such as interviews and focus group discussions rely on nurses’ self-report on nursing practice (Braun & Clarke, 2014; Creswell & Creswell, 2018; Krueger & Casey, 2015). This study highlights the potential for systematic observation to enhance understanding of capability development and whether postgraduate education further enhanced new graduate capability. This is the second paper reporting findings from a doctoral study that investigated different approaches to a new graduate programme; one that included a postgraduate course versus one that did not. The first paper reported on the impact of completing a post graduate course in clinical assessment on the capabilities of new graduate nurses (Doughty et al., 2021). In this paper we report on the research findings of using systematic observation to ascertain the demonstration of capabilities in practice and to evaluate new graduate nurse capabilities in a real-world context.
BACKGROUND
Systematic observation of practice offers important insights into nursing practice that may not be captured in participants’ self-reports. Bryman (2016) referred to structured observation as “a method for systematically observing the behaviour of individuals in terms of a schedule of categories” (p. 267). Structured observation is also known as systematic observation (Michaels, 1983), and the term systematic observation will be used throughout this article. Systematic observation can be used in both qualitative and quantitative research and is a method of obtaining data in various research designs (Andrew & Halcomb, 2009), by observing participants going about activities in their natural setting. The purpose is to record behaviours, actions and interactions (Andrew & Halcomb, 2009; Schneider et al., 2008), the qualities of which are both complex and subtle and not possible to fully discern in participant self-report, such as in questionnaires. What individuals say about their performance may not correlate with how they act. Self-report can be considered imprecise because it is subject to various response biases (such as responding in a manner believed to be socially desirable), which can distort a person’s account of actual performance (LoBiondo-Wood & Haber, 2018). However, self-report is not invariably inaccurate, nor is observation necessarily free from response bias or distortion (Kazdin, 2020).
Social research has various dimensions of observation depending on the researcher’s involvement. These include structured observation (also known as systematic observation), participant observation, non-participant observation, unstructured observation, simple observation and contrived observation (Bryman, 2016; Creswell & Creswell, 2018). Observing nurses in practice, and how they respond in real time is an important adjunct to participant self-report. Compared to questionnaires and interviews, systematic observation provides greater precision regarding the timing, duration and frequency of particular practice situations, behaviours and events (Bryman, 2016). Systematic observation is applied in other contexts in nursing, so it is familiar in this field (for example, it is used in simulation training and education) but has not been employed to evaluate new graduate nurse capabilities. When combined with data about nurses’ perceptions of real-world scenarios, systematic observation can provide a powerful adjunct to the extant literature on nursing capabilities and help us elucidate the how and why of questionnaire-based findings. There is a notable gap in understanding what practice capabilities look like and also in comprehending new graduate nurses’ perceptions of their capabilities.
What is systematic observation of practice in research?
Systematic observation is a way of obtaining data by observing participants going about usual activities in their natural setting while maintaining an unobtrusive presence as possible (Bryman, 2016). In the context of nursing, it involves observing nurses caring for patients, and for our particular study, the focus was their practice in hospital settings. Participants are observed for a predetermined period, with the purpose to record behaviours, actions and interactions (Andrew & Halcomb, 2009; Schneider et al., 2008), the qualities of which are both complex and subtle and not possible to fully discern in participant self-report, such as in questionnaires. Behaviours are usually recorded using an observation schedule/tool which specifies the categories to which observations should be assigned (Bryman, 2016).
Systematic observation allows researchers to determine if, when and how often behaviours of interest occur in practice and may reveal environmental influences on individuals’ reactions to certain situations. Systematic observation in nursing research is not used as widely as other research methods, possibly in part due to the time commitment but also the challenges faced in setting up, gaining consent, gaining access to the clinical environment and executing the research (Salmon, 2015; Twycross & Shorten, 2016).
As with all research methods, systematic observation has strengths and limitations (Table 1). The strength of systematic observation is that it can capture what people do and how and why they react as they do. As a method, systematic observation has the potential to address the gap between inferred and actual behaviour, recording actual behaviours and noting any omissions that may have been mentioned in a self-report (Bryman, 2016). Being able to capture the changing nature of contextual factors, such as the unpredictability of the practice environment, patient acuity, how the nurse reacts and how this informs nurses’ practice and clinical decision-making, is a strength of systematic observation (Gillespie, 2010). Challenges of systematic observation may include between-observer reliability, where multiple observers are involved in ensuring consistency in applying the tool to record behaviours/practice. In these instances, employing a structured observational tool with clear operational definitions is essential and can avoid the tendency to generate imprecise data (Bryman, 2016). An operational definition is the statement of procedures used to measure a specific variable (Karimi et al., 2016), or capability factor in our study. The more precise the operational definitions, the more reliable the data (Michaels, 1983). Observer experience and expertise are an additional consideration; familiarity with capabilities and nursing practice, in general, is important.
METHODS
A multi-method doctoral research study using systematic observation was conducted to investigate the influence of two different approaches to a new graduate programme on the development of new graduate nurse capabilities, one including a postgraduate university course and one without such a course. The delivery of these programmes have been described elsewhere (Doughty et al., 2021).
Objectives
The aim of undertaking systematic observation in practice in our study was to:
-
identify the extent to which new graduate nursing capabilities are observed in practice
-
determine whether including postgraduate nursing education in a new graduate programme enhances the development of new graduate nursing capabilities.
Study design
Systematic observation was used to assess new graduate nurses during completion of their first year of practice and the New Zealand national Nurse Entry to Practice (NETP) programme. This observation methodology captures nursing practice during two separate 30-minute periods of continuous recording over one 8-hour shift. Each observation period was followed by a 15-minute debrief session.
Setting and participant recruitment
This research was conducted in two large metropolitan hospitals in Aotearoa New Zealand. Directors of Nursing from the two study sites granted permission for the researcher to complete systematic observation onsite and for the new graduates to be contacted to invite them to participate in the research. The new graduate programme coordinator at each site sent an email to all new graduates who completed questionnaires, inviting them to participate in observation of their nursing practice and a post-observation debrief session. The email invitation included the participant information sheet and consent form. A convenience sampling approach was used, whereby the first four new graduates from each site who indicated their willingness to participate were recruited, resulting in eight new graduate participants in total. All new graduates were working in similar medical and surgical areas at both sites, further enabling comparison of their practice. Observation of eight new graduates was anticipated to provide sufficient data to generate meaningful insights, ensure study feasibility, and reduce the burden on the setting and patients.
Patients being cared for by the participating nurses during the observation period were also asked to sign a consent form indicating they were aware that their nurse was being observed but they were not, and that no information was being collected about them. To remove potential researcher bias or coercion, the NETP programme coordinator approached patients to gain consent.
Data collection and instruments
Eight new graduate nurses participated in the study. Data were collected over January and February 2019. All measurements were taken by the lead author who is a registered nurse and experienced in the adult acute care nursing practice setting. Ethical approval was granted by the University of Auckland Human Participants Ethics Committee (ref. 022152); informed consent was gained from all participants in this research.
Systematic Observation
An observation framework was designed based on the work of Bell et al. (2012). The framework focused on four key capability factors identified in the initial phase of the wider research programme: knowledge for practice, explaining practice, confidence in practice, and applied diagnostic reasoning (Doughty et al., 2021). Operational definitions and examples of behaviours indicative of each factor in practice were identified by the authors with collective professional experience in nursing practice (Table 2). When developing a tool for systematic observation, it was valuable to draw on the 4D&4R tool (Rollans et al., 2013). The 4Rs “react, respond, real-life experience and reflect” indirectly informed the tool to investigate the dynamics of interactions between the new graduates and their patients in the context of developing capability. The framework followed a systematic non-participant observation process, meaning the researcher observed the new graduate nurses in practice but did not participate in the clinical activity at any stage (Bryman, 2016). An event recording process that enabled the observer to document each time the new graduate nurse engaged in a target behaviour associated with capabilities of interest was preferred over duration recording (Floyd et al., 1998).
Piloting the observation tool
The observation tool was piloted to test its reliability and identify any practical concerns about how the data was recorded, ensuring the data accurately represented practice (Creswell & Creswell, 2018). The pilot was conducted at a separate hospital not involved in the main research project. The pilot participant was a nurse who met the same characteristics as the study participants (completing a new graduate programme) but worked at a hospital separate from the two research sites. This nurse participated only in the pilot testing phase of the research. A university nursing colleague, not associated with the research in any other way, assisted the researcher with piloting the tool by simultaneously observing the nurse in practice. The recording of behaviours on the observation tool was then compared, and minor changes were made to the content structure and formatting of the tool.
New graduate systematic observation
It was important that participants felt prepared whilst undergoing observation in practice, careful planning ensured the process was ethical and comfortable for both the nurses and the researchers. The participant information sheet informed new graduates about the research study prior to consent. Prior to commencing the observation, the researcher reiterated that they had the right to withdraw from the observation of practice at any time without reason. The researcher also reassured the nurses that the observation would be as unobtrusive as possible, and they would remove themself during any intimate patient cares.
New graduates were observed in their work setting during two separate periods of 30-minutes of continuous recording over one 8-hour shift to capture the nature and diversity of their work over a standard clinical shift. The observation tool (Supplementary File 1) was set up to record the occurrence of specific behaviours associated with each capability. A tick was placed on the observation tool when behaviours associated with a specific capability were observed, and examples of practice to support the observation were noted in the comments column of the observation tool. For example, one indicative behaviour for knowledge capability states, “demonstrates behaviour that suggests a level of knowledge relevant to patients’ presenting condition.” An example of practice associated with this capability was observed when a new graduate was asked to check a controlled drug, and the new graduate questioned an incorrect drug dosage, demonstrating pharmacological knowledge. Data collection commenced 15 minutes after the observer entered the practice setting to allow for habituation (Mulhall, 2003).
New graduate nurses’ reflections
Following the observation period, a 15-minute debrief session was undertaken with each new graduate, led by the researcher. All conversations were audio recorded and transcribed verbatim for analysis. Discussions centred on critical reflection of the new graduate practice during the period of systematic observation, focusing on their perspectives on what went well for them during the session and what didn’t go so well for them. Participants were also invited to share any other perspectives about the observation period, their day overall, and completing the new graduate programme.
Data analysis
For the systematic observation, data counts of capability indicators were calculated at an individual level and means, medians and ranges were calculated across two setting groups and postgraduate (PG) education status (Group 1 [+PG] had completed PG nursing education; Group 2 [-PG], had not completed postgraduate nursing education). A qualitative descriptive approach was used to analyse qualitative new graduate response data from the debrief sessions (Polit & Beck, 2021). Data analysis used a deductive semantic approach whereby findings were generated from data provided with no additional meaning attributed to comments made by participants (Braun & Clarke, 2022). This approach was deemed most suitable given the structure of the data collection and the brevity of information provided by participants.
RESULTS
As is common when reporting observational data, graphs and tables have been used to report the within-group (Figure 1) and between-group findings (Figure 2) for 235 observed behaviours.
To what extent are new graduate nursing capabilities observed in practice?
The individual nurses (four +PG and four -PG) demonstrated varying capabilities across the four factors: knowledge for practice, explaining practice, confidence in practice, and applied diagnostic reasoning. Two hundred and thirty-five behaviours associated with the four capabilities were observed across the eight nurses. Seven nurses had similarities in knowledge for practice, with one nurse (Nurse 7) notably showing fewer behaviours across this factor (Figure 1). There was a consistent pattern where the same nurse demonstrated fewer instances of behaviour across the other three factors. Two nurses (Nurses 4 & 5) demonstrated the lowest count of behaviours in the factor explaining practice, with both having demonstrated knowledge for practice. Behaviours that indicated nurses’ confidence in practice were more common; the level of confidence appeared to reflect the level of knowledge whereby nurses demonstrating more behaviours in knowledge for practice scored higher in confidence in practice. This was also the case for the nurse showing the lowest count of behaviours for knowledge for practice and demonstrating fewer instances of behaviours for confidence in practice. The largest difference between the eight individual nurses was noted in the applied diagnostic reasoning factor, which was observed more frequently in the four nurses completing a postgraduate course than in the four nurses not completing such a course.
In Figure 1, confidence in practice for new graduates that completed postgraduate education appears to be related to their applied diagnostic reasoning. New graduates who did not complete a postgraduate course had a high level of confidence in practice, but this was not reflected in applied diagnostic reasoning (Figure 1). Pearson’s r correlation coefficient was used to measure the strength of the linear relationship between confidence in practice and applied diagnostic Reasoning. Pearson’s r correlation was .44 and a p value of 0.14 indicated no significant correlation between confidence in practice and applied diagnostic reasoning. This indicates that confidence in practice does not necessarily translate to the capability of new graduates to applied diagnostic reasoning in observed practice.

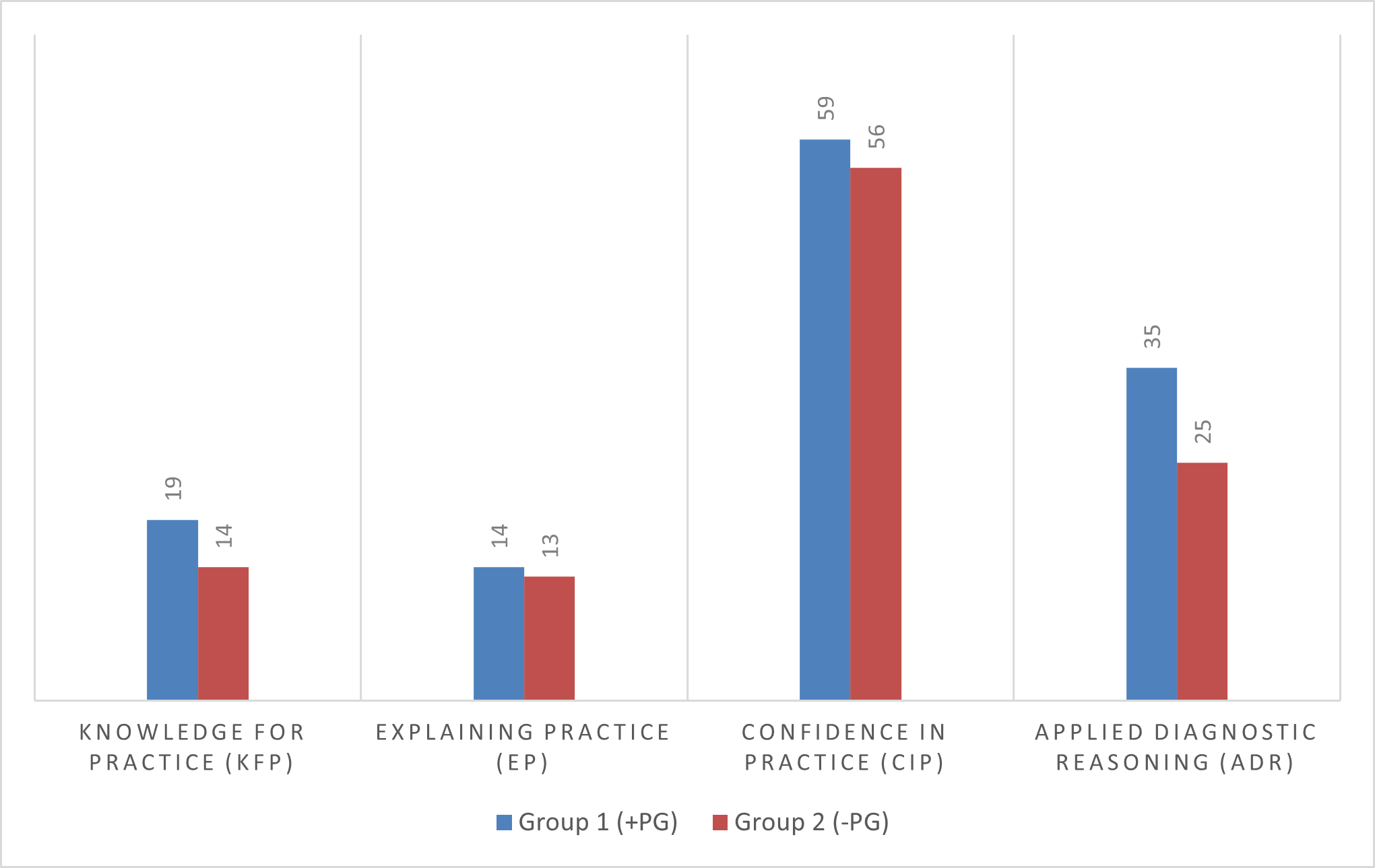
Both groups demonstrated capability across all four capability factors. It is not meaningful to compare instances of behaviours across factors as the opportunities to demonstrate the indicated behaviours may have varied. Still, given that the nurses worked in similar settings, opportunities were expected to be similar. However, it was noted that the number of observations for each group across three named factors, knowledge for practice, explaining practice and confidence in practice, was similar. Group counts for factors were compared with confidence in practice, which accrued the highest counts overall. The lowest counts were for explaining practice. The largest difference between the two groups was noted in the applied diagnostic reasoning capability (Figure 2). Examples of observed behaviours in practice within the four capabilities are shown in Table 3.

Does including postgraduate nursing education in a new graduate programme enhance the development of new graduate nursing capabilities?
The mean, median and range for both groups across the four capability factors are presented in Table 4 The mean scores for explaining practice between both groups were similar as was the mean score for both groups in the confidence in practice. There were obvious differences across two factors, with Group 1 having a higher mean for knowledge for practice. The largest difference was for applied diagnostic reasoning, where Group 1 had a notably higher mean compared to Group 2 (Table 3).
The following example demonstrates applied diagnostic reasoning capability of new graduate nurses (+/- PG). The patient relayed that she felt very dizzy each time she stood up:
NG (+PG) took the patient’s blood pressure lying/ standing to consider postural hypotension;
NG (-PG) took the patient’s blood pressure and said it was within normal parameters. The nurse didn’t consider taking lying and standing blood pressures.
New graduate reflection supplements insights into new graduate capabilities
The debrief sessions provided an opportunity to listen to the new graduates’ reasoning about their practice capabilities and highlighted that new graduate nurses thought completing the new graduate programme enhanced their capabilities (Table 5). The examples they shared supported the behaviours observed during systematic observation, illustrating a deeper understanding of new graduate practice. New graduates referred to some additional examples that were not directly related to capability development. The new graduates identified unrealistic workloads and the impact on their ability to perform the holistic functions they identified with the registered nurse role. All new graduates also alluded to postgraduate study in some way and spoke positively about engaging in future studies. Group 1 new graduates were glad to have had the opportunity to undertake further study at a postgraduate level but were also looking forward to a break from study. New graduates from Group 2 (-PG) saw the value of completing a new graduate programme but did not comment on formal postgraduate study during the programme. This may have been because a postgraduate course was not included in their new graduate programme.
DISCUSSION
This small observational study, which was part of a larger doctoral research programme, set out to identify the extent to which new graduate nurses’ capabilities were reflected in practice. Systematic observation allowed insights into new graduate practice not evident through self-report questionnaire only. Findings indicated that while all new graduates demonstrated behaviours reflective of four capability factors, Group 1 (+PG) new graduates demonstrated more instances of the capabilities of knowledge for practice and applied diagnostic reasoning, which are highly relevant to contemporary clinical practice in complex environments (Herleth et al., 2020).
These findings concur with previous survey-based findings, which showed a significant increase in new graduate capabilities of knowledge for practice, explaining practice and applied diagnostic reasoning for new graduates who had completed postgraduate education during their new graduate programme (Doughty et al., 2021). Undertaking systematic observation of new graduates enabled a first-hand account of actual practice behaviours (Twycross & Shorten, 2016).
A strength of this research is the triangulation of data sources, including new graduate clinical practice observations, a post-observation debrief session, as well as the ability to address the limitation of self-report by systematic observation in practice. Findings from this study aligned with previous research showing that undertaking observation in the clinical environment has real value and research potential (Jackson et al., 2016). Examples provided throughout this paper have demonstrated that systematic observation of new graduate practice and interaction with colleagues revealed the decision-making and attitudes embedded in everyday clinical practice that were not captured solely through self-report questionnaires.
It is important to further consider the value of systematic observation as a research method. Nursing is currently facing many challenges, particularly around attrition in Aotearoa New Zealand and internationally (Brook et al., 2019; Ministry of Health, 2019; World Health Organization, 2020). Clinical environments have become more challenging over recent years, given the dynamic nature of healthcare and the increasing complexity of the patients’ needs (Jamieson et al., 2023; Ortiz, 2016). Systematic observation can capture the complexity of the clinical environment, with both predictable and unpredictable events being captured in real-time.
The unpredictable nature of practice demonstrated how new graduates were required to make clinical decisions in uncertain and rapidly changing environments. Systematic observation of new graduates provided evidence of capability and the associated influence of the environment. It also offered insight into how new graduates’ knowledge informed their clinical reasoning in making decisions regarding patient care. Observing how new graduates engaged with the patients and explained care provided evidence of knowledge and confidence capabilities.
Behaviours associated with knowledge for practice and applied diagnostic reasoning were observed more in new graduates having completed postgraduate education. This suggests that including postgraduate education in a new graduate programme may provide a more supportive context for capability development. Behaviours associated with confidence in practice were the highest scored factor across all individual new graduates, with both groups appearing confident in their practice towards the end of their new graduate programme and this was also reflected in the post-observation debrief sessions. The confidence levels between both groups were similar, which may be attributed to completing the new graduate programme. This finding is consistent with literature which alluded to confidence as a dynamic process that develops over time (Ortiz, 2016), as new graduates consolidate their learning and build their capability (Walker et al., 2017). Confidence in practice for new graduates who completed postgraduate education appears to be related to their applied diagnostic reasoning. New graduates who did not complete postgraduate had a high level of confidence in practice, which was not reflected in applied diagnostic reasoning. However, statistical analysis did not indicate this difference was significant.
Postgraduate education has been shown to impact nurses positively, predominantly in the advanced nursing workforce and those working in speciality areas (Baxter & Edvardsson, 2018). There is limited evidence regarding the impact of postgraduate education on new graduate nurses (Doughty et al., 2018; McKillop et al., 2016) and minimal regarding new graduate capability development (Doughty et al., 2021). The findings reported here concur with previous literature that claimed postgraduate education produces a workforce that can confidently articulate and apply their knowledge to inform their evidence-based clinical decision-making and diagnostic reasoning in practice (Hickman et al., 2018; Massey et al., 2019).
Findings from this study are novel and have added to our current understanding of new graduate capability development. The main strength of systematic observation is that it provides direct access to actual new graduate nursing practice to record observed behaviours. Systematic observation revealed how and why new graduates responded as they did in observed situations revealing decision-making, clinical judgements and attitudes reflective of capability development as a valuable adjunct to self-report.
The integration of the findings reported here with new graduates’ self-ratings of capability in a separate component of the research (Doughty et al., 2021) has added new insights into the impact of completing postgraduate education on new graduate capability development. In particular, it has indicated, even though not statistically significant, that new graduates completing postgraduate education did display more instances of knowledge for practice and applied diagnostic reasoning capabilities than new graduates who did not complete postgraduate education. However, it is not possible to know whether the differences were setting and workplace-related or related to the postgraduate education completed during the NETP programme. These findings may inform future decisions regarding the optimal timing for new graduates’ to pursue postgraduate education, shaping the trajectory of their professional development.
Observational studies undertaken in hospital settings have unique ethical challenges since they occur in clinical practice environments, in which patients may be involved (Fry et al., 2017). There are limitations and uncertainties given the complexities of the environment and the unpredictable, fast-paced comings and goings that unfold throughout the day. This challenge is reflected in one period of observation where the observer noted multiple fast patient turnovers, acute admissions, ward transfers, transfers to theatre and discharges – rich in detail but challenging for new graduates; this level of data collection would not have been captured in a survey response.
Informed consent is a fundamental principle of all ethical research (Twycross & Shorten, 2016). Systematic observation requires identifying who will request consent from participants so as to minimise bias or coercion. There is also the ethical obligation (Nursing Council of New Zealand, 2012b) to raise any concerns about issues of unsafe practice, wrongdoing, or risks witnessed (Nursing Council of New Zealand, 2012a) that could endanger patients or others during the period of systematic observation. A clear process of reporting was put in place that any event causing concern and potential harm to patients would immediately be reported by the researcher to the charge nurse on duty at the time.
Despite the challenges, systematic observation can lead to a better understanding of nurses’ practice and the decisions and clinical judgements they make, rather than sole reliance on self-report measures, providing us with richer data to examine every day clinical nursing practice (Salmon, 2015; Twycross & Shorten, 2016). Employing systematic observation in nursing research can answer questions about how nurses respond to different situations, and the data collected can generate new knowledge that is not always evident in other methods.
Limitations
Systematic observation may involve a relatively small sample size, however, the unit of measure in this research was each recorded behaviour of which there were 235 observed. There is always the potential for bias with just one observer, involving multiple observers allows unbiased generalisation. This is something to consider with future studies involving observation.
The Hawthorne effect, whereby a participant’s behaviour may change due to being observed, can cause a dilemma for the researcher. The researcher waited 15 minutes from entering the practice setting before commencing data collection to allow for habituation. It quickly became evident to the observer that the nurses were too busy to maintain behaviour radically different from their usual practice.
CONCLUSION
Clinical practice is highly complex and technical; nursing is patient-centred, holistic, and humanistic, and using systematic observation as a research method can focus on new graduate nurses’ practice behaviours, individual uniqueness, and stresses. It can take account of how social, cultural, and working environments may influence experiences and individual behaviours. Systematic observation can capture or inform the researcher as to the how and why of nurses’ everyday practice and reactions.
This research has added insight into real-time nursing practice, not easily accessed in other research methods. Given its value and research potential, it is worth overcoming the possible challenges of undertaking systematic observation in the clinical practice setting. This study provides valuable insight into the benefits of undertaking systematic observation and the value for further research using this method. It will hopefully encourage others to consider systematic observation as a research method to evaluate nursing capability in the clinical environment.
Acknowledgement
Thanks to all participants who contributed to this research
Funding
None
Conflict of interest
None