INTRODUCTION
Self-employed nursing is an unusual career choice in Aotearoa New Zealand (NZ). Self-employment provides the opportunity for nurses to continue their contribution to health and nursing and create a work environment that is both professionally satisfying and personally fulfilling (Sanders & Kingma, 2012). The number of self-employed registered nurses (RNs) in 2018, the year of data collection for this study, was 1.8% of the total nursing population (Nursing Council of New Zealand, 2019). In 2018, only 24 RNs identified as being self-employed in the practice area of professional advice and policy (Nursing Council of New Zealand, personal communication, February 26, 2019). Globally, there is a deficit of policy-based nurses (World Health Organization, 2020). Nurses working in policy are critical in developing strategy and policy advice on workforce, models of care and service delivery (Manning & Krieble, 2020; Sanders & Kingma, 2012). This study focuses on nurses working in professional advice and policy at local, regional or national level in Aotearoa (NZ).
Nurses can offer a particular expertise in policy roles because they have a broad view, across the whole of health. However, decision-making at local, regional and national level is often undertaken without nurses (Manning & Krieble, 2020). Manning and Krieble (2020) observed that nurses are rarely at ‘the table’ where health policy and funding decisions are made, advocating that the ‘table’ needs to change. In the meantime, they recommend that nurses need to learn the language of policy, and the machinery of government (Manning & Krieble, 2020).
To inform RNs about the opportunities to work in non-traditional nursing roles in non-traditional workspaces, it is valuable to learn how others have coped with disruption, financial challenges, new opportunities, and working from home. The Nursing Council of New Zealand (NCNZ) (2007) competencies for professional advice and policy provide a helpful structure and starting point for nurses considering or entering this practice area and include, but are not limited to, project manager, nurse consultant, policy analyst and quality advisor. The focus of this study was to explore the experiences of RNs (the participants) transitioning into and practising as solo self-employed contractors within the practice area of professional advice and policy.
BACKGROUND
To raise the voice of nursing and to be around the policy and decision-making tables, it is important to understand how the participants adjust to non-clinical roles in non-clinical spaces. The predominant focus of nursing research is clinical practice and nursing education and while there is a dearth of empirical research pertaining to nurses who work in the practice area of policy, there are two exemplars of policy research. Stahlke Wall (2011) used focused ethnography to explore all types of self-employment in nursing, but predominantly clinical. The participants had all previously been hospital employees and once in self-employment found themselves balancing a business focus with nursing values, which created financial precarity and at times, isolation. Wilson (2003) used a Delphi technique to explore the experiences of 54 nurse entrepreneurs in Australia. The tensions of professional isolation, financial precarity and access to funding were all found in this mostly clinical participant group. Findings of both studies found marginalisation and financial worry associated with moving from being an employee with a guaranteed salary to being a self-employed nurse with an erratic income.
Nurses typically spend a substantial portion of their early career as employees, but there are experiences that create the impetus for change into non-clinical self-employment as contractors (Sanders & Kingma, 2012). These are known as push-pull factors and include restructures, burn-out and lifestyle choices. Push-pull is a long-established concept (Sasso et al., 2019; Wall, 2014) used in reference to workplace behaviour (Hughes, 2003; Ministry of Women’s Affairs & Ministry of Economic Development, 2008) and is a useful way of identifying why nurses change roles. For example, a push factor could describe feeling pressured into leaving an untenable role, whereas a pull factor could represent the desire to move to a more rewarding lifestyle (Manning, 2022). The concept of agency is important for nurses shifting to self-employment to realise a sense of control over their working life (Vanucci & Weinstein, 2017). Wilson (2011) suggests that nurses choosing self-employment will often have strong agentic positioning with specific experience, motivation, networks, and transferable skills-sets.
The lead researcher (EM) has experienced the move to policy-based self-employment. She has been an independent nurse consultant and contractor for 13 years. Prior to starting the research, she had experienced dissonant reactions when explaining not only her non-clinical work context but that she also worked from home. EM regularly experienced comments such as, “Nurses work in hospitals and how can a nurse become a doctor [of philosophy]?” This combined with a sense of marginality, both professionally and geographically, working in areas of grey, being financially precarious and having to learn new skills in running a small business, all prompted the study. EM describes that the study and findings have been life changing, giving access and insight into her own personal and professional interiority (being and identity). Finding comfort in remaining in a liminal space, between typical nursing employment and self-employment, together with a feminist approach has supported both practice and professional positioning. EM’s personal experiences suggest that unwrapping the previously unspoken complexities, tensions and contextual factors navigated in self-employment shows that communication skills, advanced practice, adaptability and professional agility become highly developed.
METHOD AND METHODOLOGY
This study used focused ethnography, a new and flexible ethnomethodology, which evolved from traditional anthropological ethnographic methods, first described by Knoblauch (2005). Focused ethnography is variously described as micro-ethnography, mini ethnography and ethno-nursing, due to the frequency of its use in nursing (Holloway & Galvin, 2017; Polit & Beck, 2012; Roper & Shapira, 2000; Streubert & Rinaldi Carpenter, 2011). It benefits from the researcher’s own insights as a member of the group being studied through an insider or emic perspective, by delivering a level of pre-understanding for a deeper probing of the topic (Berger, 2015; Brannick & Coghlan, 2007; Holloway & Galvin, 2017; Polit & Beck, 2012; Wall, 2015). Using interviewing and flexible participant observation, focused ethnography suits a solo researcher and is an effective way of documenting perspectives and cultural changes within a group (Holloway & Galvin, 2017). It uses an inductive approach (Roper & Shapira, 2000) and has flexible requirements for participant observation. It also uses episodic participant contact when required, rather than traditional ethnographic approach of cultural immersion (Knoblauch, 2005).
Theoretical perspectives: Liminality theory and gender theory
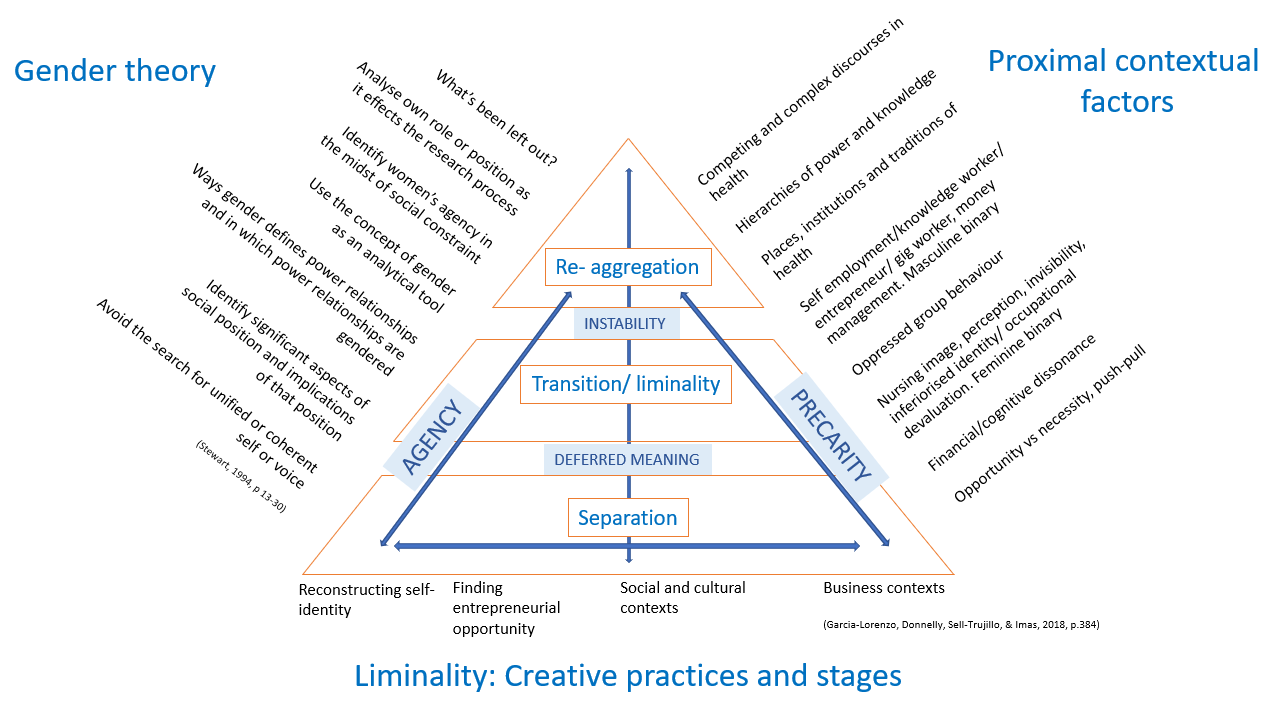
Liminality theory was originally described in 1909 by van Gennep (1960), and focused on a cultural rite of passage, or a specific life transition however, this was based in a Eurocentric patriarchal approach. The concept has been revisited several times (Czarniawska & Mazza, 2003; J. C. Turner et al., 1987; V. Turner, 1987). This study required a contemporaneous model of liminality theory. Garcia-Lorenzo et al. (2018) presented “Creative practices of liminality” which identifies the three phases of liminality through which nascent entrepreneurs in self-employment move: 1) separation from the known identity; 2) transition through a period of uncertainty and readjustment; and 3) the integration of a new identity. Liminality has been described through the years as a life process, often with fluid phases but always with an ending (Czarniawska & Mazza, 2003; J. C. Turner et al., 1987). Garcia-Lorenzo et al. (2018) introduced the concept of continuous or enduring liminality for some aspects of self-employment and is supported by other recent works (Ibarra & Obodaru, 2016; Willis & Xiao, 2014). This approach aligned closely with the researcher’s (EM) sense of her work as a self-employed contractor.
Nursing is a gendered profession (Eliason, 2017). In Aotearoa (NZ) and globally, the vast majority of nurses are female (Mitchell, 2017; Nursing Council of New Zealand, 2019) and in terms of socially accorded values, the masculinities are privileged and the femininities disprivileged (Bhakuni & Abimbola, 2021). Gender research can reveal how social constructs can be powerfully positioned to create privilege and disprivilege (Vuolanto & Laiho, 2017). Gender theory is an appropriate lens to view the occupationally and binary stereotyped nursing profession (Busch, 2018), particularly for nurses who are moving into a masculine space of business and policy (Scott & Scott, 2021) while working from the domestic sphere of the home.
Participants
Participants were recruited from across Aotearoa (NZ) by accessing relevant national nursing networks using purposive and snowball sampling (Minichiello et al., 2004; Polit & Beck, 2012). Participants were required to be RNs and self-employed criteria included working as solo self-employed in a full time or part-time capacity and with no other employment income. Thirteen were recruited and all were experienced RNs (from 15 years to approximately 40 years), with current practising certificates and who had worked at regional, national and, in one case, international level. Most participants had master level qualifications, one was a doctoral candidate and three already had doctorates. All the participants were female, but no further information can be given due to the small number of nurses working in this space.
Data collection
An introductory phone call from the researcher (EM) with potential participants ensured all the study inclusion and exclusion were discussed. A participant information sheet was then emailed to the participants, and an interview time was scheduled. Data collection was through semi-structured interview (Holloway & Galvin, 2017) and observation of the environment in which the participants worked. Given the limited literature on nurses in policy or as self-employed contractors, the entrepreneurship competence framework (EntreComp) (Bacigalupo et al., 2016) was drawn upon to develop interview questions. The framework intends to cover entrepreneurship across all spheres of life, including personal development, participation in society, employment opportunities, and starting up new ventures (Bacigalupo et al., 2016). The three key competence areas are: ideas and opportunities; resources; and into action. Under each area there are further competencies, for example, spotting opportunities (ideas and opportunities), mobilising resources (resources), and taking the initiative (into action).
Data analysis
This paper reports on the analysis of the interview data. Data were manually analysed (Braun & Clarke, 2013; Holloway & Galvin, 2017) using thematic analysis which required frequent and detailed review of all data to enable reduction, merging, coding, and mapping into subgroups and then main themes. Themes were constructed through critical analysis, and then considered in more depth using the theories of liminality and gender to capture the complexity in which the participants worked. The theoretical and contextual framework (Figure 1) was developed drawing on the theoretical frameworks of liminality (Garcia-Lorenzo et al., 2018) and gender and the proximal contextual factors from the literature review. The intent of the framework was to capture the complexity of the environment in which the participants were positioned: geographically, professionally, experientially, socially, creatively, contextually and liminally (Manning, 2022). Using the framework throughout the analysis process ensured rigour and that complex spaces, hierarchies, gendered binary approaches and liminal theory were consistently considered.

Ethics
The study was approved by the Massey University Human Ethics Committee (NOR 17/59). Participation was voluntary and verbal consent was gained prior to interviews. The participants were informed about confidentiality and anonymity of identity, roles, and locations, a particular issue in this study as there are so few RNs working in the relevant practice area as self-employed. Study pseudonyms were chosen by the participants. Written consent was obtained at the interview. Digital audio and video recordings were transcribed under a confidentiality agreement between the researcher and the transcriber.
FINDINGS
Thematic analysis revealed three key themes: 1) Push-pull: used in this study to describe the employment choices and actions the participants made when faced with work-life challenges or opportunities; 2) Finance and business: the participants needed to learn new skills such as how to invoice and the requirements of owning a business and the challenges of charging a reasonable contract rate were also confronted; and 3) Public and private: the participants had moved from a public clinical space where nurses traditionally work, to the private domestic sphere of a home office, where their role was not always clearly defined.
Push-pull
The participants in this study chose self-employment and this section outlines their thoughts on leaving salaried employment and their reasons for doing so. The phenomenon of push-pull was evident in the data, including the push factor of frequent restructures:
Having been through significant restructures, having been in my role for 15 years as a [senior RN] as well. I still loved that job but finally the fourth disestablishment it was, “Well now is the time for me to be really thinking about what else I want to do with my life.” [Jeanette]
A loss of confidence in employers, restructuring and budget cuts created momentum for a push into self-employment:
I ran into a kind of roadblock at the [organisation] I had worked at for years and lost faith in the leadership, in terms of following due process, and that led to me feeling unable to do my job. [Sally]
There is evidence of Jeanette and Sally’s long-term commitment to their previous employers which suggests that the decisions to leave were not easily or quickly made.
The following participant evinced the pull-factor approach to self-employment having had career-long salaried roles:
Freedom, I would say, would be the biggest – the sense of freedom. And the autonomy. I’d always had a hankering to one day be self-employed. So, it’s the realisation of a dream and the dream was a mixed portfolio, and I’ve certainly got that. [Jessie]
Jessie equated self-employment to freedom, so while the overall direction is ‘pull’ there was an implied escape from something more structured to a more varied work-life on her own terms.
Finance and Business
Most participants were embarking on self-employment for the first time which meant a precarious financial situation was a new experience. Data illustrated that even for highly skilled senior RNs, an erratic income, learning to invoice, charge a contract rate, and dealing with the Inland Revenue Department (IRD) made this transition extremely uncomfortable at times. Tash recounted the dreams she had that evidenced how disruptive the transition had been:
But the nightmares were really interesting. Well, they weren’t nightmares but there was just this image I had of getting into business, having this big mortgage and being homeless. You know the images of refugees that are fleeing, and they’ve got their old people in wheelbarrows, and I had visions of me and [partner] destitute with [mother-in-law] in a wheelbarrow; like nowhere to go and homeless. [Tash]
Revealing her anxiety in vivid images, Tash was relating a real fear, that her family would suffer, and her business would fail. The anxiety of financial failure was reasonable as there was a risk of significantly lowered or even no income:
I’ve had months where I’ve not invoiced anything - generally January, February, the long summertime holiday is generally very quiet. [Billie]
The quiet of the summertime, while not necessarily unusual did show that being liminal to the workforce may result in less work over quieter times. To explore mitigation approaches in response to erratic income, the participants were asked whether they had marketing strategies:
Marketing, not very good at it, because again it’s about touting for work and, it’s all wrapped up in that package of “How much you are going to pay me?” [Billie]
Marketing was avoided by virtually all the participants. The dichotomy of wanting work but not wanting to advertise undermines the visibility of this valuable but small workforce and positions them liminally. However, data reflected that advertising may not be required in all circumstances:
I basically just get people coming to me and the odd proposal, if I hear about it and I go for it, and I do that. But I haven’t really got much into the cold calling. You don’t need to. Actually, if you’ve got networks, meeting for coffee and lunch reminds them that you’re around and that’s enough. [Susan]
Participants identified that networks are the principal way of finding work for this niche group:
Probably what helped was that when I first started, I already had strong national networks and when I was a nurse in [city] I’d been on a couple of national boards and knew people across the country in different roles. I had a lot of those links before I started which really helped. [Jill]
This example reinforces the view of the participant group, that networks and word of mouth have primacy in finding contracts. However, most participants did not have marketing experience to draw from as a comparison.
A vital area of business acumen is invoicing an adequate fee for services. However, this was something most participants found challenging because they had to have self-belief in their own value:
It does feel strange invoicing people. Because what you’re saying in some ways is, “I’m really rating my ability here. I’ve got something that you don’t have, and I’m charging you for it. So, I’m feeling fairly confident that I’m giving you something that’s going to help you.” So, you have to be in that space, you do have to rate yourself. [Lou]
The participants would frequently invoice based on a contracted hourly rate plus GST, and this rate could be perceived as a higher rate than anything RNs in salaried employment would receive. However, Nancy described the reality:
But, absolutely there’s no appreciation, that actually what my hourly rate is only a third, because I pay my own GST and I pay my own tax. If I’m sick I don’t get paid. If my child’s sick I don’t get… you know, none of that. [Nancy]
The data provided examples of increased understanding of the additional considerations which RNs must factor into a contract fee, though charging a fee for service remained an uncomfortable space for many of the participants.
Most participants reported that the steepest learning curves involved in financial management were learning the intricacies of GST (goods and services tax) and the requirements of the IRD:
So, I do think you have to be really, really, disciplined about how you make sure that you never, ever get into financial strife. The last thing you ever want is any trouble with the tax department. [Jessie]
There was a degree of fear and concern about the potential for making financial mistakes and the punitive late fees applied by the IRD. To avoid any issues with paying tax, the participants had strategies in place, such as that described by Jayci:
I learnt that no matter what happens you do not interfere with what you’ve got put aside for tax and put it in a separate account and earn interest on it and sit there and watch it for six months. [Jayci]
The participants found managing the financial aspects of self-employment challenging, but only because they had no experience to draw on. Once they understood the process, they became competent:
So, I’ve made sure that I’ve built up a good reserve in my company so that I never have any trouble with the tax department and have a buffer if I became unwell. And I’ve got that reserve really protected. And I’ve kept contributing to my super [superannuation] and my KiwiSaver [pension] and all those sorts of things in readiness for 65. But all of them would be a protection if something untoward happened. [Jessie]
While the participants reported they had become financially literate for business, most continued to struggle with surmounting the challenge of charging reasonable contract rates and earning a realistic income.
Public and private
The participants moved their work and workspace to the private space of the home. A family home is not the traditional space where nursing identities are performed. The participants described gendered challenges around space and barriers, which required negotiated family engagement for business success but, while based in the gendered space of home and liminally positioned the participants found their leadership skills were still in demand.
Data indicated that the move to a home office may have the unintentional consequence of being caught in a web of gendered compromises in trying to blend work and the private spaces of the home. For some this required a negotiation for space:
Whenever we need the table for meals, when there is four or more of us, I have to tidy up my space and move my things elsewhere until after the meal is completed. [Jeanette]
It is significant to note that although participants highlighted the shift to contract work was driven by the desire for greater freedom, the reality brought new disruptive compromises to be navigated daily. For some the claimed space was temporary, and the family took priority. Other participants had created a permanent space in the family living room:
The office is in our living room, so I would call that stifling the need for creativity and space. Eventually, I’d like to have a sleep-out or something outside that is the office, rather than the office being in the living space. But it is what it is. We have two desks in our living space, and we manage and it’s fine. [Sally]
The impact of having workspaces in the family’s living space created issues relating to noise, interruption, privacy, and the ability to concentrate:
Given I work in an open-plan living area there are no physical barriers. However, I will go to another room to make and receive phone calls if anyone else is at home. If I have a planned call or teleconference in my diary, I will let my family know so that they realise I need quiet during that period. [Jeanette]
The use of barriers required the agreement of the entire family in some cases, which was negotiated to ensure understanding and compliance to sustain the business communications and professional networks in that space.
Data showed that participants considered it important to continue to contribute their leadership skills in ongoing relationships with nursing colleagues and networks. Participants considered that these continuing connections added to the sense of success of their self-employed endeavours. Examples were supporting colleagues, provision of supervision and mentorship, or being sought out for advice:
The people I work with now can get really stuck with things. I’ll say, “Well, have you thought about this?” or, “In my experience, this could work quite well,” and the joy is immense. Because they might have had to go round the block a few times to get there. So that’s a great feeling, and that’s helping. I’m still in a helping role. [Lou]
The move to self-employment saw the participants remaining liminal in the competing spaces of home and work, nursing, and self-employment. However, they all remained connected to nursing networks, and adopting helping roles was a source of professional satisfaction, considered a measure of success.
DISCUSSION
The contribution of this study is to illuminate a little-known career option, that of self-employment in the practise specialty of policy. The data reflected the challenges met as the participants made the transition into solo self-employment. They had demonstrated internalised views and beliefs about the nursing profession. Despite these constraints they were challenging the way RNs can practice, how RNs are financially valued and where RNs work.
The participants used their agentic positioning to leave a difficult employment situation or to actively seek an improved work-life balance and freedom. Sanders and Kingma (2012) describe that motivation to be self-employed requires “vision, a creative idea for solving a problem, and a strong desire for success” (p. 23). Seeking change illustrates the initial separation phase of liminality theory as described by Garcia-Lorenzo et al. (2018). While the concept of push-pull was used to describe the triggers for their decisions, each participant’s situation was far more complex and emotional, with tensions concerning separation and beginning their journey into self-employment. For example, participants had not anticipated the new compromises that would arise, and nor had they anticipated the sense of vulnerability they experienced due to financial precarity.
The participants were also confronted with their own and others’ views of their monetary worth, described by Busch (2018) as occupational devaluation. The study participants appeared to be somewhat constrained by the vestigial notions of nursing as a feminine vocation (Busch, 2018). As similarly found by Wall (2013), attending to issues such as negotiating direct payment were viewed as unpalatable. These concerns were combined with a distaste for marketing and self-promotion. Traditional gendered views impacted detrimentally on being successfully self-employed and saw virtually all the participants significantly undercharging for their expert services (Sanders & Kingma, 2012; Wall, 2013).
Mitigating financial risk was a concern for the participants. Generally, RNs are salaried employees with a regular income. Moving to an erratic income, with the potential for months with zero income was a risk. The current study found that participants used two methods to mitigate their financial risk: accountants or friends and family. Blackburn et al., (2018) found that accountants can be a positive influence in managing finance and reducing associated anxiety, particularly in relation to tax requirements. Sperber and Linder (2018) suggest that help can also be found in family and friend networks, where experience in business or accounting can support day-to-day decision-making and simple tax issues. The participants also chose accountants who were women, which Ahl and Marlow (2012) suggest could be a way to avoid being measured against traditional standards for business success. The general view of success was being asked to participate in leadership, to be approached to give advice, and continue to contribute, rather than making more money.
In the current study, becoming a self-employed non-clinical RN created unforeseen challenges, particularly when participants elected to work from home. The dynamics of working from home post-COVID, when it became more acceptable (Bick et al., 2020; Combe, 2020), requires further exploration. However, self-employment paired with workspaces in the gendered domestic sphere found some participants routinely acquiescing to family assumptions about their availability or negotiating for space. Work based tensions in the home can be improved by what Allen et al., (2020) define as boundary management, including explaining the work to friends and family, setting time, physical and noise barriers and where possible creating a permanent workspace.
CONCLUSION
In their move to solo self-employment as a contractor in policy, the participants experienced challenges, personal stresses and at times, financial precarity. They became liminally positioned, professionally, and geographically, but were able to act agentically to realise their talents, networks, and expertise. While it is unlikely that solo self-employment in policy will suit no more than a small minority of RNs, it is no less valuable.
Contemporary nursing practice in Aotearoa (NZ) offers a myriad of non-clinical pathways for nurses which are largely unknown by nurses, but the profession has an opportunity to expand the conventional view of RNs and nursing. The study has shown that RNs with the relevant expertise can create spaces and practices to best suit their skills and experience. However, for RNs to become successfully self-employed, in a professional advice and policy specialty, they must face previously unrecognised vocational ideas that constrain them in articulating their value.
Funding sources received
None.
Conflicts of interest
None.