INTRODUCTION
Nurse staffing is a critical element in the efforts to ensure patient safety and improve outcomes. However, there is no gold standard approach to decisions around safe staffing requirements (Griffiths et al., 2020). Specific to the operating room (OR), the Australian College of Operating Room Nurses (ACORN) argue that adequate numbers of appropriately qualified and experienced nurses are essential to the safe and effective care of patients in the perioperative environment (ACORN, 2014).
Operating room nurse managers have known for some time that approaches used for staffing inpatient care units, such as wards, are not an appropriate model of care for the OR (Barratt & Schultz, 1997). Inpatient care delivery units typically use a budget-based model (Burrows, 2018), patient/nurse ratio model (Burrows, 2018; Olley et al., 2018), or a patient acuity calculation model (Meyer et al., 2020; Nursing Advisory Group, 2022), which do not reflect intraoperative care requirements. Instead, OR staffing models of care have traditionally been based on the number of ORs and sessions available for surgery (Barratt & Schultz, 1997). However, there are concerns that this staffing methodology fails to consider the nursing resources thought to be important for safe, high-quality patient care.
Within existing perioperative literature, recommendations for safe staffing are vague. A scoping review incorporating international and local (Aotearoa New Zealand) literature (Taylor, 2021) identified that terms such as “adequate” (Marenzi & Nelson, 2009, p. 31) or “sufficient” (Murphy, 1994, p. 1064) were used when referring to safe staffing. When discussing skill mix, authors of included articles indicated that OR nurses needed to be “competent to fulfil their assigned duties” (Murphy, 1994, p. 1064), without providing a clear definition of what the term competent meant. There was no agreement in the literature on what was considered to be safe OR nurse staffing resource. In Aotearoa New Zealand, national perioperative nurse staffing recommendations are based on international recommendations (Perioperative Nurses College [PNC] of New Zealand Nurses Organisation, 2022). However, the research evidence supporting these recommendations and their suitability to the Aotearoa New Zealand healthcare environment was unclear. Consequently, this study explored OR nurse staffing decision-making processes and practices in Aotearoa New Zealand. We aimed to identify factors senior perioperative nurses consider when making decisions about nurse staffing and skill-mix. The research questions were:
-
How do senior nurses describe safe patient care in the OR?
-
How is nurse staffing and skill-mix determined for safe patient care in the OR?
-
What are the resources and processes used to make staffing decisions?
METHODS
We used a qualitative descriptive study design (Sandelowski, 2000). The study was set in two major public hospitals in an urban centre in Aotearoa New Zealand providing surgical care services ranging from simple to very complex procedures. Inclusion criteria were senior nurses who make decisions about nurse staffing in operating rooms providing perioperative services for both acute and elective operating lists. Recruitment was via an emailed invitation from OR managers of the two sites, which included the participant information sheet, consent form and interview guide. Potential participants contacted the researcher by email or phone to arrange an interview time and place.
Semi-structured individual interviews were used to explore nurses’ perspectives on how decisions were made about safe nurse staffing in the OR. Interview questions were informed through a scoping review of the literature (Taylor, 2021) to determine how core concepts of safe patient care and nurse staffing decision-making in the OR were described (for example, Association of periOperative Registered Nurses [AORN], 2021; Bell, 2015; Gilbert et al., 2011; Siirala et al., 2016). Questions were piloted with a senior nurse from the researcher’s (BT) hospital to ensure they were open-ended and broad enough to encourage participants to share their views on the topic without researcher influence (Creswell, 2014). Demographic data were also collected to enable us to understand the context in which staffing decisions were made. Interviews were conducted in February and March 2020 by BT, an experienced OR nurse. Interviews were uninterrupted and conducted on-site, in private, quiet rooms within the participants’ own departments.
Interviews were audio-recorded and transcribed verbatim. Braun and Clarke’s reflexive thematic analysis process was used to analyse the data and generate themes (Braun et al., 2014; Braun & Clarke, 2006, 2020). Analysis followed a six-phase process that involved familiarisation with the interview transcripts, generating initial codes and themes from the data in relation to the research question, reviewing, defining and naming themes and then production of the research report (Braun et al., 2014; Braun & Clarke, 2006). The study design was developed with consideration of Lincoln and Guba’s evaluative criteria for establishing trustworthiness (Lincoln & Guba, 1986; Schwandt et al., 2007).
The collection and analysis of data were informed by the primary researcher’s (BT) perspective on safety, developed from working in the perioperative environment for over 20 years. BT used this experience to probe further into topics during interviews, enabling insight into participants’ unconscious decision-making processes and adding further depth and breadth to data collection and analysis. BT was careful to reflect on her personal views throughout the execution of the research project, ensuring that the themes presented were data-driven. As per the evaluative criteria suitable for qualitative descriptive methodology (Schwandt et al., 2007), peer-debriefing and the use of verbatim quotes promoted trustworthiness and credibility of the data analysis.
Ethics approval for the study was obtained through the Auckland Health Research Ethics Committee (AHREC:AH1061) and locality approval obtained from the organisation chosen for the setting. Informed consent was obtained from all participants.
RESULTS
A total of seven (n=7) interviews were conducted with experienced senior nurses (Table 1). The majority of participants were clinical nurse managers (CNMs) (n=6) responsible for the staffing of between four and seven specialty ORs within their department, each with a team of nurses and healthcare assistants (HCAs) who were managed and deployed each day. Participants’ years of nursing experience ranged from 18 to 43 years (median 22 years). The length of time they had worked in their role (such as making decisions about nurse staffing) ranged from one year to 11 years (median eight years). All participants trained in Aotearoa New Zealand (n=7). Participants (P) P1 to P4, came from Hospital A and P5 to P7 from Hospital B.
Themes
Four themes relating to safe OR nurse staffing were constructed from the interview data: 1) safety: team-based, person-centred care; 2) the importance of skill-mix; 3) safe staffing: ‘Not just about the numbers’; and 4) the complexity of staffing decisions. Within each theme were various subthemes (Table 2). The themes were interdependent, multidimensional and intertwined, with each theme contributing to the next, together building a view and understanding of the provision of safe perioperative nursing care and the complexity of OR nurse staffing decisions.
Safety: team-based, person-centred care
It’s not only about knowing what the surgery is, or what you’re doing, it’s an innate skill and ability to hear what’s happening, to see what’s happening, and to consider ‘Okay, I know this person has…’ [P4]
This theme relates to how the senior nurse participants defined safe patient care in the OR. The essence of this theme is that the notion of safety encompasses all aspects of the individualised patient care that the perioperative nursing team provides. This theme is complex, having many subthemes related to both the holistic care of the patient having surgery and teamwork within the OR.
Critical thinking: Nursing skill, knowledge and experience
All participants held the view that perioperative nurses were essential for patient safety in the OR. Nurses were described as using their foundational knowledge and building on this with specialised nursing knowledge of surgical specialties, the OR environment and intraoperative patient care. Critical thinking was regarded as crucial for patient safety:
You can train monkeys to be theatre nurses, but all they do is function in the physical capacity of a theatre nurse. They don’t have the critical thinking. They don’t have the background to assess patient’s clinical conditions and interpret them. [P7]
Examples of the importance of critical thinking in nurses’ practice included completing the pre-operative checklist that encompassed individualised risk assessment and the application of in-depth knowledge of operations and anaesthesia that enabled nurses to anticipate intraoperative safety issues and respond swiftly and appropriately in emergency situations.
Leadership and teamwork
Participants believed perioperative nurses contributed to safe patient care by simultaneously providing leadership and actively engaging in teamwork during surgery. They described nursing leadership as important for safe care, with nurses both leading and working effectively within the team as they participated in activities promoting patient safety, such as preparing the OR for the next patient, completing safety briefings and solving problems that, if unresolved, could result in adverse patient outcomes. Participant 1 stated: “I always say no-one’s going to be able to walk in without our nurses because they organise everything.”
Effectively working as a team also meant teaching other team members. As such, senior nurses were considered crucial to safe patient care when new or junior registrars were assigned to lists without direct support from a consultant surgeon. One participant clearly linked this teaching role to a core aspect of patient safety, stating that:
If it was a junior registrar that had just come across on a rotation, then I would really want some senior leadership in there to assist him. [P6]
Amongst other things, participants described how senior and other experienced nurses managed the day-to-day operational management of the individual OR with its list of patients. These nurses ensured everything ran smoothly and efficiently, solved problems and resolved issues whilst also providing guidance and support for the team:
And she [senior/experienced nurse] is generally the one that’s overseeing the whole running of the theatre; the timing, the equipment, making sure they’ve got everything available, making sure the team’s supported in there. [P5]
Professional responsibilities
Participants further described professional nursing responsibilities they considered important for safe patient care. Examples related specifically to nurses’ role responsibilities that could not be delegated to other members of the OR team. For example, participants spoke of nurses ensuring all instruments and supplies used during surgery were accounted for at the end of the procedure, maintaining the sterile field, and managing traffic in the OR to reduce the risk of post-operative infection. Accountability for the practice of the staff they were supervising, was also a specific professional responsibility:
As a registered nurse, you’re accountable for the practice of healthcare assistants, enrolled nurses, student nurses, [and] new grads. [P7]
Patient comfort and care
Participants described providing comfort and support to patients throughout their journey as a key aspect of safe nursing care, equating patient-centred care to safety. Examples of this care included taking the initiative to welcome the patient and family/whānau on arrival to OR, providing support, advocacy and explanations of what was going to happen:
And if we’re not there with the patient side by side, we’re explaining to them what and when we’re doing things. [P3]
Other examples included, ensuring that patients were kept covered with blankets to keep them warm and the consideration of emotional and spiritual needs by providing reassurance, comforting talk and touch:
They [nurses] recognise patients need to either pray, cry, take a breath, have another question or [need] another conversation with a surgeon. The nursing staff will be there to support. [P4]
Cultural safety
This subtheme is about ensuring patients’ cultural beliefs and personal preferences for care were respected throughout their perioperative experience. All participants identified that all staff are expected to provide culturally safe patient care as part of safe practice. Specific examples of culturally safe care described by participants were supporting family/whānau presence in the pre-operative area and ensuring that patients had the opportunity to have their body tissue returned to them if that was their preference:
And that’s part of the conversation that you’d have with them. ‘Would you like these returned to you?’ and Yes? ‘This is how. We’ll do it for you. This is the process. And we’ll make sure it’s all documented in your notes’. Yeah. It’s a whole complete package. [P6]
Physical safety
A final aspect of this theme is participants’ description of ensuring the physical safety of the unconscious patient and protecting them from injury in ways critical to patient safety. For example, ensuring correct patient positioning to prevent pressure injuries and keeping patients’ limbs safely secured and padded against pressure were regarded as an essential nursing responsibility. P4 described that if, for example, a procedure usually takes 90 minutes, then physical safety will include “safe positioning and pressure relief area” [P4].
The importance of skill-mix
Leading by example and showing the novice nurses this is how we do it, this is what we need to do to ensure our care is exemplary for our patients. [P6]
This theme related to the importance of nursing skill-mix for safe patient care in the OR. Building on the previous theme, the essence of this theme was that one of the highest priorities when deciding how best to allocate nurses was ensuring the right skill-mix for each case to secure the provision of safe and appropriate patient care. The analysis identified that OR nurses could not be considered as all the same, as a wide range of nurses’ skills, qualifications and qualities were described. Participants linked skill-mix to the knowledge and experience of the individual nurse and their skills and abilities within surgical specialties. Participants specifically spoke about skill-mix using Benner’s (1984) levels of practice, describing the progression of the different levels in relation to the care provided by the nurses and their level of responsibility within the OR. Each level of nurse contributed to safe staffing in a different and distinct way.
Stages of proficiency of registered nurses
Participants described expert nurses as being experienced and knowledgeable within the surgical specialty as well as being an essential resource for the rest of the nursing team. Senior and expert nursing support within the OR was considered to be critical to ensuring safe patient care, as it provided leadership to other nurses and coordination of the multi-disciplinary team. P3 reflected how expert nurses “tend to [have] the accountability and the confidence in patient care, and leading the [whole] team” [P3].
Eight qualities of senior/expert nurses were generated from participants’ descriptions of senior nursing practice. Nurses with the following qualities were considered pivotal to the safe running of the department: leadership skills and accountability; communication skills; knowledge, clinical skill and experience; ability to manage stressful situations and problem solve; efficiency and organisational skills; observation, awareness, anticipation and preparedness; superior critical thinking; teaching skills and ability to support others. It was senior nurses’ ability to embed these qualities into their daily practice that stood out as a significant contribution to OR safety. For example:
We know that should any complications arise, they [senior/expert nurses] will be the right ones to be able to manage in those situations, because at that point in time, there will be quite a stressful situation in theatre. [P2]
Another participant stated:
I’d have someone that would be in there that would be able to get the flow of the theatre going, rather than… You still want the theatre to move as opposed to not move, and I find sometimes when I have somebody like a [senior/expert nurse] in the theatre they will do five cases, as opposed to a non-[senior/expert nurse] where I’ve got two cases done. [P3]
Participants described proficient nurses as having developed knowledge and experience within a surgical specialty, understanding the surgical requirements of their specialty cases, and of how the OR runs. Proficient nurses were described as able to provide a level of leadership, however, they still required support from the CNM or other senior nurses. While competent nurses were described as not needing to be “the standout person” [P1], they were described as capable nurses able to work independently. Finally, new graduate nurses, as novices, were still developing and focussing on the immediate task they were responsible for completing.
Enrolled nurses
The participants discussed the value of having experienced enrolled nurses (ENs) in the OR. Enrolled nurses were described as working interchangeably with registered nurses (RNs), performing the same roles (i.e. scrub nurse and circulating nurse) as RNs. Participants spoke of the EN limitations (accurate to the EN scope of practice at the time of data collection), such as not taking a leadership role in the OR and “the legalities” [P2] of accounting for equipment and swabs because, “two enrolled nurses cannot do a count together. It has to be registered nurse” [P2].
Safe staffing: ‘Not just about the numbers’
I’ve always said that in every operating theatre, you need three nurses. One who knows what they’re doing all the time. One who knows what they need to do most of the time. And one that might not necessarily know everything, but they’re willing to learn. [P7]
This theme relates to the importance placed on nursing staff allocation for safe patient care in the OR not being solely based on the number of nurses. The essence of this theme is that allocating the appropriate number of nursing staff to each OR is important, however, it is not as simple as it sounds. This theme follows on from the previous, where it was clear that not all nurses were equal with respect to ensuring safe staffing decisions. Whilst participants agreed that they planned on allocating three nurses per OR based on the standard model of care, staffing numbers were increased or decreased depending on multiple factors, such as nursing experience and skill-mix, individual case requirements, the availability of staff and the need to develop new staff, emphasising a key finding that safe staffing is not purely about the number of nurses in an OR.
Three Nurses?
Participants explained that they started planning with the three nurses as their usual standard of staffing, which was based on fulfilling the three perioperative nursing roles defined by participants as the anaesthetic nurse, the scrub nurse and circulating nurse. They explained that staffing an OR with three nurses was not merely about having the roles filled, but also ensuring an adequate balance of experience for safe patient care and, as illustrated in the quote above [P7], supporting the skill development of new staff.
Two Nurses?
Whilst all participants agreed that having three nurses was the ideal model of staffing, several participants gave examples where it would be appropriate to have two nurses, one of which must be an RN, usually with a dedicated HCA to provide support. The reasons given for having just two nurses in an OR included having skilled experienced nursing staff, not needing a scrub nurse and/or having less complex cases. However, participants also indicated that the OR was less efficient and less productive when there were two nurses, potentially resulting in delays for those patients later in the operating list, with the potential that they might be cancelled. Participant 7 described:
[If] there’s only two of you, you’re probably only going to get four maybe five [operations] done. So rather than cancel the whole list… it is better to have three nurses on.
A broader organisational view of safety was therefore also apparent, with participants very aware of the need to complete the operations of all patients on the list for that day and doing their best to prevent cancelling operations.
Four or more nurses?
Multiple examples were given where participants felt additional nursing resource was required to safely staff an OR. Examples included complex and long cases, fast-moving surgeons or surgical lists, cases that required two teams, cases that required lots of equipment and supplies, and the need to teach and train nurses. Decisions about how many nurses were required to safely staff an OR were based on considering the specific case requirements:
The reality is, you know, we allocate three nurses to a theatre and then depending on whether there’s more involved, we’ll look to see who else we can pull in to there. [P1]
The complexity of staffing decisions
It is dependent on the patient acuity. The complexity of the case. And also, the multiple comorbidities the patient might have. So, those are all the factors that we take into consideration, and also the experience of that individual nurse. How he or she would be able to manage that list effectively. [P2]
This theme is intended to capture the complexity of staffing decisions, requiring consideration of a myriad of factors relating to each individual patient, nurse, list, OR session, and the team as a whole. The factors are categorised under general principles.
Balancing the skill-mix available
Given previous themes, it is unsurprising that all participants identified that one of their most important considerations when making staffing decisions was the safest and most appropriate balance of nursing skill-mix across the department. Participants described ensuring they appropriately allocated the senior nursing staff, whilst also considering how best to assign the proficient, competent, new graduate or novice nurses, ENs, and HCAs rostered for that shift. Participants spoke about assigning nurses to individual ORs to ensure that the mix of nursing practice levels was allocated across the department in the safest possible way, trying “to have an equal balance of skills - the skill-mix between the theatres” [P2].
The right nurse for the case
Additionally, all participants agreed that finding the best fit of nurses to the cases or surgical lists was important. Participants described matching the skills of individual nurses’ knowledge and experience with the type and complexity of the operation, the acuity of the patient, the surgical equipment required, and the caseload. Participant 6 explained:
It’s just not a matter of ‘Oh, I’ve got this and this and throw those people in there’, you’ve got to consider what skills people have. [P6]
Supporting the team
Another core principle when safely assigning staff was how best to ensure the team is supported, thereby reducing stress and burnout, especially for the more junior and learning nurses:
I think safe staffing is a priority of all nurse leaders. Because what we’re trying to avoid is burnout among staff and we have to be mindful of that. [P2]
Flexibility
Participants also described how having the flexibility to move staff across specialties facilitated safe staffing. Even with the best long-term planning, flexible and fluid staffing decisions supported a safe response to the inevitable changes in the daily case mix and staff availability. Flexibility also enabled senior nurses to safely accommodate surgeries for patients coming in acutely:
“And I think the advantage on this side is that our staff are quite flexible. They can work in different specialties, especially in the acute ORs, we expect them to have that flexibility.” [P2]
Operational considerations
Commonly, participants described how planning for cases started weeks in advance, reflecting the multiple operational considerations impacting nursing staff allocation. On the day, staffing decisions were finalised to ensure the appropriate mix of skills for the complexity of planned cases and specialty requirements for the safest care of patients. This process involved consideration and collaboration with other charge nurse managers about how best to utilise the team of nurses available, as illustrated below:
But generally the day before is when we go, ‘okay, what’s going into that theatre’, because everything’s been locked in, and then we can say, ‘okay, these are the people [nurses] we want in there’. [P1]
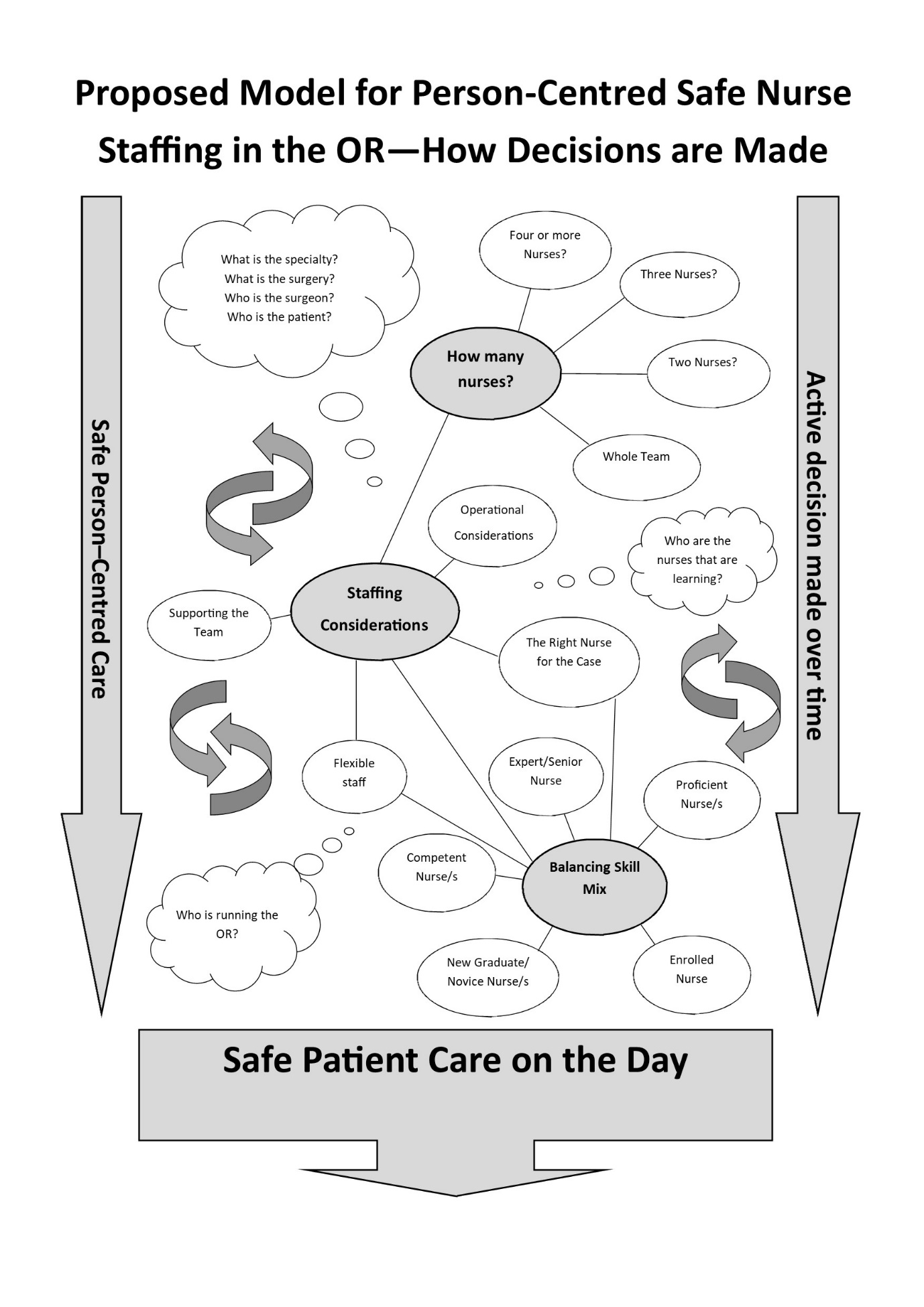
Nursing knowledge framework for person-centred, safe nurse staffing in the operating room
A ‘Nursing knowledge framework for person-centred, safe nurse staffing in the operating room’ has been constructed from the themes identified in this research (Figure 1). This framework illustrates the complex and integrated factors involved in OR nurse staffing decisions, as described by senior nurses in this study. It is intended to guide those involved in safe staffing from within the OR to management levels. The framework provides a structure to consider the multiple and dynamic factors influencing safe patient care in the OR on any given day. Depicted in the framework is how planning for safe nurse staffing begins weeks prior, when surgical lists are initially proposed, and then how planning continues over time with consideration of all factors within each theme right up until the day of the surgery. Continual assessment of all factors is a necessity, given that staff availability and case mix often change initial decisions regarding the best deployment of nursing staff.

DISCUSSION
This study aimed to identify factors senior perioperative nurses considered when making decisions about nurse staffing and skill-mix. Through the analysis of seven senior nurses’ perspectives, working in perioperative care, we identified four themes central to their decision-making to achieve safe staffing. Theme one, safety: team-based, person-centred care, revealed how participants focussed on delivering individualised safe patient care. This theme underpinned and gave context to the other three themes generated that collectively provided the link between safe nursing care delivery and staffing allocations. Theme two, the importance of skill-mix, established that one of the highest priorities when deciding how best to allocate nurses is ensuring appropriate skill-mix for each case to secure provision of safe patient care, including senior nursing support within the OR. Theme three, safe staffing: ‘not just about the numbers’, identified that OR nursing staffing allocation is not purely about following a numbers-based model of care. Theme four, the complexity of staffing decisions, adds other factors senior nurses considered when making OR nurse staffing decisions.
Our findings indicated that a ‘numbers’ approach to staffing is unsatisfactory for ensuring staff and patient safety in the perioperative environment (Figure 1). The complexity of OR nurse staffing decision-making indicated that decisions were not a simple or straightforward allocation of ‘three nurses per OR’. Rather, key factors were considered, such as nursing experience, the mix of skills, the complexity of procedures, delivering patient-centred care, and staff availability. Staffing plans adjusted over time, spanning from the moment charge nurse managers learnt about planned cases until surgery was completed. However, no tangible resources or formalised decision-making processes were described by participants; rather, they relied on their personal experience and consultation with peers to make decisions.
The importance of incorporating nurses’ experiential and professional knowledge into nurse staffing was evidenced in a meta-narrative review identifying that nurses are best placed to articulate what they do and how their work supports patient safety (Jackson et al., 2021). These findings are consistent with McKelvie’s doctoral research, conducted in Aotearoa New Zealand to evaluate the Care Capacity Demand Management (CCDM) acuity-based staffing programme. The CCDM programme was implemented in response to the 2006 Safe Staffing Healthy Workplaces Committee of Inquiry Report, which identified strategies to address concerns that hospitals were inadequately staffed to meet the increasing complexity of patients (Nursing Advisory Group, 2022). McKelvie (2019) found that the “substantial and significant professional situated knowledge” (p. 244) was missing from the nurse safe staffing tools, reiterating the risk to patient safety when staffing and patient acuity are reduced to numbers (McKelvie, 2019). This evidence, alongside our findings and similar work identifying the complexity of safely staffing in radiology services (Freebairn et al., 2022), signal the importance of safe staffing guidelines that reflect the unique environment of the OR, and value the knowledge and experience of senior nurses within those environments.
Participants in the study agreed that having at least one senior/expert nurse or an experienced proficient nurse in each OR was an essential element of safe staffing. As such, nurses cannot be considered to all have the same level of knowledge and skill, which is entirely consistent with descriptions in the New Zealand Perioperative Nursing Knowledge and Skills Framework (PNC, 2016). Additionally, participants identified that novice nurses were allocated as additional to the core nursing team until they developed competence, which has been described elsewhere in the literature (Matapo & Kennedy, 2020; Wilson, 2012; Wu & Taylor, 2020).
Allocating nurses with the appropriate skill, knowledge and experience best suited to each OR was a key element in the nurse staffing decisions identified in our study. This finding supplements existing evidence arguing that staffing allocation decisions are made based on areas of responsibility and the competence and skills of nurses (Bell, 2015; Siirala et al., 2016). However, our results also showed that staffing factors were individualised for each patient, list and OR session, indicating that decisions around the safe allocation of nursing resource are based on both the skill and experience of the available nurses and the individualised care needs of each patient. Previous literature has discussed decision-making concerning nursing staff allocation to the ORs (Faulhaber, 1991; Fisher, 2011; Siirala et al., 2016). However, no studies were able to provide insight into the decision-making around how nurses were allocated to individual ORs.
Interestingly, participants described instances where they were comfortable decreasing perioperative nurse staffing resource (from three to two), for example for more straightforward operations. They also described situations where more nurses were required. This nuanced way of deciding staffing allocation is not reflected in international nor Aotearoa New Zealand staffing recommendations and guidelines (AORN, 2021; ACORN, 2014; PNC, 2022; Woodhead & Fudge, 2012). Participants also described the need to occasionally run ORs with less than their preferred complement of nursing staff to prevent cancelling patients’ operations. Such efforts to maintain organisational productivity are described in the literature and can be viewed as a threat to patient safety (Alfredsdottir & Bjornsdottir, 2007). Furthermore, expectations to do more in less time is leading nurses to feel under pressure, risking burnout (Al Zamel et al., 2020). Instead of standardising OR nurse staffing levels, it is more important to be able to adjust numbers according to case complexity and patient acuity (AORN, 2021; Bell, 2015; Gilbert et al., 2011) and ensure a balance between organisational productivity and nursing burnout.
Overwhelmingly, was the determination to provide individualised patient care, as described by all the senior nurses in the study. A qualitative study exploring nurses’ views on patient safety found that having comprehensive knowledge of each patient’s individual needs was highly important to perioperative nurses (Alfredsdottir & Bjornsdottir, 2007). Similarly, Kelvered et al. (2012) identified that perioperative nurses practised person-centred care (such as individualising nursing care) to guarantee patient safety.
Significantly, our study appears to be the first to identify cultural safety as an important aspect of safe perioperative patient care. This finding is possibly unique to Aotearoa New Zealand, where the requirement to provide culturally safe care underpins nursing practice to ensure healthcare equity for Māori (the Indigenous people of Aotearoa New Zealand) under Te Tiriti o Waitangi (Nursing Council of New Zealand [NCNZ], 2011a). In practice, the senior nurses in this study were committed to providing culturally safe individualised nursing care and commented on the need to include whānau and support wairuatanga (spirituality) throughout the perioperative period. The NCNZ has recently released Proposed Registered Nurse Competencies (NCNZ, n.d.). Although the proposed competencies are still under consultation, they now have a strong emphasis on Te Tiriti of Waitangi and the provision of culturally safe care, supporting the work perioperative nurses currently provide in this aspect of their practice, and also the potential to do more. Cowles’ (2024) recent research provides welcome insight into the practical application of Māori values in a perioperative setting.
Strengths and limitations
This study is the first to investigate factors considered when making decisions about safe OR nurse staffing in Aotearoa. A strength of this research was the purposeful choice of a sample of subject-matter experts. The participants, senior perioperative nurses, possessed an in-depth understanding of OR nurse staffing deployments and the complexity of acute care, enabling them to provide rich, deep data, supporting information power despite the small sample size (Malterud et al., 2016).
A potential limitation is that data were collected from just two hospitals in an urban setting Aotearoa New Zealand. However, the broad range of OR specialities and depth of nursing experience represented suggests these results are transferable to settings similar to those described. An important limitation is the absence of Māori participants, which has meant a limited view on what culturally safe OR staffing looks like and implications for honouring Te Tiriti o Waitangi in this setting.
Implications for nursing management
The results from this research provide important insights into what informs nurse safe staffing decisions and skill-mix recommendations by senior nurses in operating rooms in Aotearoa New Zealand. A key message is that ‘numbers’ calculations for staffing do not reflect the flexibility and agility needed to provide safe, holistic person-centred care in the complex perioperative environment.
Achieving safe staffing in the OR requires valuing the knowledge and experience of nurses in staffing decision-making. Organisational processes must reflect the context of the OR setting and be able to flexibly respond to changes.
Safe staffing models must define and clarify the meaning of ‘adequate experienced personnel’ and ‘suitably trained nursing resource’. When taking into consideration this study’s results regarding the importance of a safe mix of senior to junior RNs, it is recommended that nurses new to the perioperative environment be supernumerary to staffing requirements for a defined period of time, thus ensuring they can safely learn, and develop competency in a supportive environment.
An important practice implication is that, while HCAs are essential support staff in the perioperative environment, they should not be considered an adequate substitute for nursing staff as they do not have standardised educational preparation and are not regulated healthcare professionals (NCNZ, 2011a). Given the breadth and depth of the RN role described here, it would be a concern for HCAs to be considered a substitute for a nurse.
There is a need for further research into this topic to ensure that any perioperative nursing guidelines accurately represent the Aotearoa New Zealand population and health system requirements. The Nursing Knowledge Framework for Person-Centred, Safe Nurse Staffing in the Operating Room is proposed for guiding future work in this area.
Conclusions
This study identified factors senior perioperative nurses considered when making decisions about nurse staffing and skill-mix. Results indicated that patient safety encompasses every aspect of the individualised care that perioperative nurses provide. Decision-making for safe nurse staffing in the perioperative environment is complex, with safe patient care linked to appropriate nurse staffing allocations. It was clear that nurse staffing decisions should not be ‘numbers’ based. Factors such as nurse experience, skill-mix, case complexity, and patient acuity were core considerations of OR nurse staffing decisions. Perhaps most importantly was the recognition that to achieve safe staffing in the OR required senior nurses to be enabled within the organisation to draw on their knowledge of the complexity of the situation and decisions which promoted patient safety.
Conflict of Interest
Cynthia Wensley is an editor of Nursing Praxis. Peer review was conducted independently, in accordance with the COPE guidelines.
Funding
No funding received