
INTRODUCTION
In recognition of challenges posed by the COVID-19 pandemic, the New Zealand government approved significant monies to expand critical care capacity and capability. Funding for a 30% increase in critical care beds over a three year period was provided with a corresponding uplift in clinical staff (Beehive Govt. NZ, 2021). The demands in staffing the additional 85 beds were significant with a reported 450 additional nurses required (Longmore, 2023).
Several initiatives were funded to support development of this workforce including a 15 month nurse-led project to design, implement and evaluate a national induction eLearning programme. With a focus on clinical knowledge acquisition about the essentials of critical care, the newly termed ‘Elearning Programme (Induction) in Critical Care New Zealand’ (EPICCNZ) was to sit alongside existing local hospital/unit induction and bedside nursing preceptorship.
EPICCNZ was an ambitious national project. With a tight timeframe that required working with multiple stakeholders, it was important to develop a nationally accessible, high quality education tool that recognised local need. This paper describes how EPICCNZ was developed and implemented, and details critical lessons learnt.
BACKGROUND
As for many countries, COVID-19 brought new challenges to critical care in Aotearoa New Zealand. Prior to COVID-19, critical care was already experiencing capacity pressures. With high numbers of patients needing critical care admission early in the pandemic (Bravata et al., 2021), the relative low numbers of Aotearoa New Zealand critical care beds was perceived as a major concern (Young et al., 2021). In highlighting the need for greater pandemic preparedness, this resulted in major government funding to expand capacity and capability in Critical Care in Aotearoa New Zealand.
Internationally, critical care areas were also responding to the pandemic by rapidly increasing both bed and staff capacity. To enable rapid surge workforce induction at scale, in-service training became an important focus in preparing new staff, especially nursing staff (Gupta et al., 2021). This was important to help build confidence in new staff about practice competencies while securing longer-term staff retention (Kiel, 2020; NHS England, 2020). Given the extent of onboarding required, e-learning induction courses were widely used across different countries (Williams et al., 2022) and settings (Alhazmi & Jamaladdin, 2022) at this time.
Use of e-learning, that is teaching and learning using information and computer technologies (Singh & Thurman, 2019), is not new in health care. On-line or web-based learning is an adaptable, accessible and convenient platform for continuing education (El-Sabagh, 2021). Nurses generally report favourable attitudes towards this mode of learning with improved knowledge and healthcare delivery outcomes demonstrated (Rouleau et al., 2019). While e-learning positively impacts on self-directed learning and learner adaptability (Adedoyin & Soykan, 2020), many factors influence its effectiveness. Limited access to computers, unreliable online learning systems and user readiness all impact on uptake of e-learning (Hayat et al., 2021). Therefore in developing a national programme such as EPICCNZ, it was important that modules were nationally accessible, engaging for new staff, clinically relevant and accurate.
PROJECT DESIGN
In April 2023, a 15-month project was initiated to design, implement and evaluate EPICCNZ. It was primarily intended for critical care nurses, although use by other critical care health disciplines and clinical specialities was explored.
The aims of the project were to:
-
develop a series of short clinical modules using multi-media accessible across the motu (island, country, land or nation)
-
engage national subject matter experts (SMEs) in e-learning, learning experience designers and capability leads to inform product development, testing and evaluation
-
use consensus methodology with key stakeholders to ensure content and consultation demonstrated representativeness and inclusivity throughout the project.
A project team was convened including a project manager (MC), National Lead eLearning in Critical Care (SJ), a core team of critical care nurses (including TK, JC) and Education Design & Technology Advisors: all based in Wellington Hospital. A Steering Group of internal and external stakeholders oversaw the project with regular reporting to Health New Zealand Te Whatu Ora. A comprehensive five phase project plan was designed including: needs assessment; programme build; programme pilot; programme implementation; and evaluation. The first four phases are now detailed, with the evaluation phase reported in a follow-on publication.
Phase 1 Needs assessment: May 2023 – June 2023
To determine current best practice, a web-based mapping of international practice about critical care induction practices and use of e-learning was completed and findings synthesised. An email was sent to 79 critical care nurse educators across the motu (island, country, land or nation) requesting copy of local induction/orientation documentation. From replies, content of 102 documents from 22 critical care areas was distilled to develop a draft outline of nine module topics and content. Content was also drawn from the shorter, more succinct and locally accessed successful SURGE (COVID-19) eLearning initiative developed by Intensive Care, Wellington Hospital.
To ensure national reach, extensive national engagement and networking was undertaken with critical care experts (nurses, allied health staff, doctors). Consultation was held with Māori, Pacific and Disability Leads across the country. Informal meetings were also held with internationally qualified nurses from one unit to understand specific challenges for nurses coming to work in Aotearoa New Zealand. Verbal and written project briefings were provided to a wide range of national professional and organisational stakeholders e.g. College of Nurses Aotearoa and national Director of Nursing forum. Links were also made with the Agency for Clinical Innovation and Higher Education Tertiary Institution in New South Wales Australia to learn from their experience of developing a state-wide critical care e-learning programme.
Phase 2 Programme build: July 2023 – February 2024
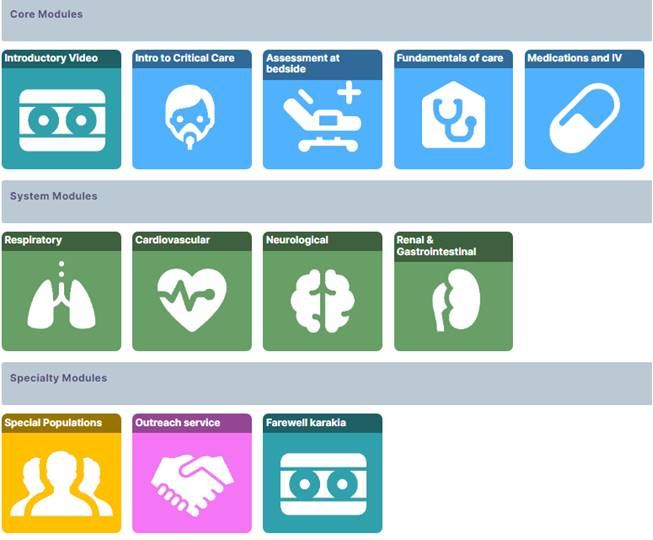
A six week sprint model (three weeks module writing, three weeks build and design) was used to develop nine modules (Figure 1). These comprised of four core modules (e.g. Introduction to critical care, Patient assessment) and five system-specific modules (e.g. Respiratory, Cardiac). Content was divided into sections detailing anatomy and physiology, conditions, monitoring and diagnostics, medications, and care and procedures.

A significant consideration in EPICCNZ was to acknowledge Te Tiriti o Waitangi (a treaty document outlining the constitutional commitment between Māori and the crown in Aotearoa New Zealand) obligations and explore cultural safety to reflect the unique Māori and non-Māori bicultural nature of Aotearoa New Zealand. Recognising Te Ao Māori worldview and applying the principles of Te Tiriti into practice are important underpinning areas in both provision of health care delivery and design of national educational health courses. There are dedicated sections in Module 1 detailing the important way of upholding the word of Te Tiriti. Furthermore, EPICCNZ opens and closes with a recorded karakia (a ritual chant, prayer or incantation to prepare for aspects of daily life such as meetings, etc.) and waiata (a song or chant, many of which belong to a group, a story, a location) provided by a kaumātua (a person of status within a group) and local hospital choir.
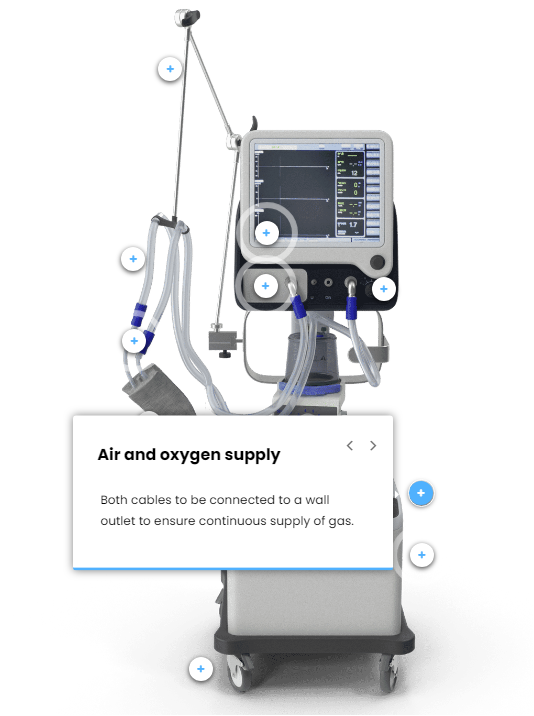
To provide an immersive and engaging learning environment, a variety of interactive tools were used throughout the modules including: quizzes, 360 photos of bed spaces, 3D anatomy models, use of hot spots (Figure 2), and drag and drop activities (Figure 3). A lightbulb symbol was used as a reminder to check local practice at key points. A red flag symbol was used to highlight key aspects of safe care. Rigorous processes were put in place to ensure only ethically-sourced photographs were used with all copyright and permissions requirements addressed. We used an attribution and intellectual property statement to acknowledge contributors and to protect their work and input. This statement underwent legal review.

As modules were developed, content was tested with national SMEs, primarily members of the New Zealand Critical Care Nurse Educator Forum (NZCCNEF – including YR) and the Allied Health Critical Care Network. Monthly e-drop in sessions were held with NZCCNEF and e-hui (meeting or gatherings) held with Allied Health disciplines. Three project-funded national stakeholder events (September 2023, November 2023, February 2024) were used to gain further module content critique and were also a focus for audio/video recording for use in the modules. Standardised questions, asked at each event, helped the project team receive feedback about content of modules while also assessing whether SMEs felt engaged with, and informed about the project. Real-time, de-identified, anonymised feedback was obtained by using Mentimeter©. Over 150 Nurse Educators, Nurse Managers and Allied Health staff attended the feedback events, and over 250 individual module feedback emails were received.

For the project team, national profiling of SMEs was important. As highlighted earlier, stakeholder events provided opportunity for ethically-consented audio/video recording (e.g. providing answers to quizzes or sharing practice experience). 18 SMEs were involved in generating this output for use across the modules. Health service users were also involved in filming including an ex-intensive care patient and a parent of a child with disability. Four additional videos were developed including an ‘Introduction to EPICCNZ’ video, two ‘mash-up’ videos of multiple SMEs giving practice advice to new staff, and a hype reel for external promotion of EPICCNZ.
Each module underwent seven different levels of review including clinical (critical care nursing, allied health, medical), quality (workforce development team and proof reading), academic (university-based adult learning expert) and technical review (Learning Design and Technical teams). This ensured content was accurate and relevant, principles of adult learning were upheld, and modules functioned correctly on the learning platforms. Reporting mechanisms were developed across each of the learning management systems (LMS) to inform the project team about module uptake and user experience.
Phase 3 Project pilot: March 2024
Piloting of all modules occurred across six sites. Twenty five staff with less than six months critical care experience were involved. Each person was allocated three modules to pilot. Standard user rating questions about knowledge, course content, and online delivery gathered feedback about the modules, with an additional 46 individual free text feedback submissions collected and analysed. This confirmed that module content was appropriate and useful, although some module completion timings required adjustment. Once the modules were ready to go live, internal technical testing of EPICCNZ occurred across one LMS before roll out and further testing occurred across all of the three national LMS platforms.
Phase 4 Programme implementation: April 2024
EPICCNZ launched on 22nd April 2024 at a national NZCCNEF conference. An extensive dissemination strategy was used with written updates prepared for all major groups and stakeholders.
DISCUSSION AND REFLECTIONS
Whilst use of elearning modules in critical care is not new (Doshi et al., 2018; Major et al., 2020; Oldenburg et al., 2019), this is the first time that a national critical care induction programme has been developed in Aotearoa New Zealand. It is interesting therefore, to compare our experiences of developing and implementing EPICCNZ with other international critical care training programmes in the COVID/post-COVID era.
EPICCNZ, similar to many courses developed, uses a blended learning approach (i.e. the course sits alongside practice) and was designed collaboratively by clinical educators, intensive care experts and frontline staff (Hettle et al., 2020; San Juan et al., 2022). EPICCNZ is a suite of modules designed to be used ‘as and when’ convenient to the learner. Sections can be omitted or repeated dependent on learner need. The ability to access content over time rather than receiving an overwhelming amount of information in one session is a helpful educational strategy (Marks et al., 2021). Each EPICCNZ module uses a range of training formats e.g. videos, checklists and simulation sessions, similar to other training (KCE Belgian Health Care Knowledge Centre, 2020; Wells et al., 2021). EPICCNZ is designed to sit alongside existing staff development strategies. This is in line with Uchida et al. (2020) who identify that practical follow-up sessions with more experienced staff are important to consolidate learning. Interestingly in our experience, feedback has indicated EPICCNZ is also being accessed by more experienced staff as a knowledge refresher and to support new staff being orientated and supported by a preceptor (an experienced companion coach).
There has been initial high uptake of EPICCNZ. Data from across the LMS identify 1193 module enrolments in the first month since go live with positive feedback from module users. When considering critical success factors for this national initiative, there are some significant stand-out areas. Dedicated funding was essential for a project manager and a small clinical nursing team to deliver on the project plan. The funding envelope gave flexibility for additional resource as project scope grew e.g. production and direction of external audio-visual content, specialist clinical input and proof readers. Funding was also pivotal to facilitate face-to-face engagement with SMEs and assist in the project being delivered in a timely manner.
Coordinating a programme of this magnitude required detailed planning to ensure timelines and deliverables were met while also building in flexibility to remain agile and responsive to changes across the programme timeline. Being able to step back and review workload and deliverables across the multiple work streams of module writing, module building, engagement strategy, quality review and evaluation, required careful monitoring. From this, timeframes were adapted or additional resource brought in, if required.
Selecting the best-fit online training software early in the project was essential. Being clear what was required of the software (e.g. look and feel of module pages, interactivity), its functionality (e.g. ability to develop and design modules within stringent timelines) and its limitations, were all important. Seeking advice from system experts and testing mock-up module pages with staff user groups informed our decision-making from project commencement.
Much time and energy was invested in the communication strategy throughout all stages of the project. We were mindful that developing a national programme could invoke concern about how local educational need would be incorporated into a national product, as well as great support about access to updated educational resource. Clear, consistent messages were delivered about how EPICCNZ could work alongside and support current orientation programmes and how use of EPICCNZ was to be determined locally. As outlined earlier, providing funding for attendance at stakeholder events as well as providing multiple opportunities for feedback ensured that EPICCNZ was fit for purpose and able to be used across the spectrum of critical care in Aotearoa New Zealand. This strategy not only ensured successful uptake of EPICCNZ but also strengthened a sense of interconnection and understanding of critical care challenges across the motu (island, country, land or nation).
Since the launch of EPICCNZ in April 2024, further modules have been developed. Module 10 (Critical Care Outreach Service) has been written and launched on 1st July 2024. Module 11 (Inter-hospital transport) is in development and due to go-live December 2024. Given modules are widely available to all staff with LMS access, we are exploring if higher acuity or specialist areas are keen to access EPICCNZ.
Finally, continuing maintenance of quality of the EPICCNZ modules is important. Processes have been mapped out for annual review with on-going governance by the Senior Leadership Team of the NZCCNEF.
CONCLUSION
EPICCNZ was delivered on budget, on time and has been well-received by the critical care community, especially by nursing staff. Bringing EPICCNZ across the line was a complex and detailed undertaking delivered by a small core team, generously supported by a substantial critical care and technical community. In this, it provides a robust benchmark for the implementation of any future national elearning projects.
Ethics
In reporting on a national service quality improvement project, formal ethics was not required. No identifiable data has been reported in this publication. In writing this paper, we have consulted and adhered to the COPE (Committee on Publication Ethics) Core Practices.
Acknowledgement
The project team acknowledge the significant contribution made by New Zealand Critical Care Nurses Educator Forum, Allied Health Critical Care Network and other medical and nursing staff involved in the quality reviews. Thanks also are extended to Māori Health Leads in TeToka Tumai Auckland, Māori Leads and Pacific Health Leads in Capital Coast and Hutt Valley, and Disability Leads in Capital Coast and Hutt Valley. We especially acknowledge the substantial work undertaken by the Learning Design and Development team especially Claire Lawson, Joe Zhou and Eric Yee, based at Capital, Coast and Hutt Valley.
Funding
EPICCNZ was supported through generous funding from the Critical Care Services Advisory Group, Health New Zealand Te Whatu Ora.
Conflict of interest
None