INTRODUCTION
As intensive and critical care services have evolved, there is an increasing focus on quality improvement, evidence-based care, and reducing the complications of intensive care unit (ICU) treatment. As a result, mortality rates in Australian and New Zealand ICUs are the best they have ever been (ANZICS, 2024; Paul et al., 2017). Whilst survival is a primary aim, there is a growing emphasis on long-term outcomes, survivorship, and quality of life for critically ill patients (Hodgson et al., 2017). Critically ill patients are typically defined as those who require specialist intensive care for a potentially reversible life-threatening condition (Kayambankadzanja et al., 2022). This highly skilled care involves the identification, monitoring, and treatment of patients with critical illness through the initial and sustained support of vital cellular and organ function (Kayambankadzanja et al., 2022). Not only are critically ill patient admissions increasing exponentially, but patients are also older, frailer, and more medically complicated (Rai et al., 2023). Complications arising from ICU treatment, including acquired infections and sepsis, respiratory failure, muscle wasting, and physical deconditioning, contribute to increased morbidity and prolonged length of stay, often requiring many days/weeks in the ICU (Darvall et al., 2019; van Heerden et al., 2020). This cohort of patients is referred to as the persistently critically ill (Darvall et al., 2019; Jeffcote et al., 2019).
The multisystem impacts of persistent critical illness on long-term outcomes are well established (Inoue et al., 2024). In 2012, the Society of Critical Care Medicine defined a constellation of physical, psychological and cognitive issues as the Post Intensive Care Syndrome or PICS (Needham et al., 2012). PICS is the result of several interrelated patient and ICU treatment factors, and not just the consequence of the initial diagnosis or disease process. Risk factors include ICU-acquired weakness, older patients with pre-existing frailty and/ or functional issues (physical component), preexisting cognitive dysfunction, sedatives, and delirium (cognitive component), lack of social support, negative experience in the ICU, and preexisting mental health issues (psychological component) (Fuentes-Aspe et al., 2024; Lee et al., 2020; Pandharipande et al., 2013; Zalta et al., 2021).
While early research on PICS has largely focused on singular outcomes or specific domains (such as cognition or quality of life), these studies often fail to capture the multidimensional burden of the syndrome on patients and their families. More recently, research has focused on the prevalence of multiple domain impacts, symptoms and co-occurring limitations. An American study found that a third of critically ill patients had cognitive impairment and depression at three and 12 months, and a quarter had functional disabilities post-discharge home (Marra et al., 2018). In an Australian context, Hodgson and colleagues (2017) studied the prevalence of disability among 262 Australian survivors of critical illness using the World Health Organization (WHO) International Classification of Functioning Disability and Health (ICF) framework (Ustun et al., 2010). They found that 25% of their cohort had moderate to severe disability at six months and only 40% had returned to work or study, with significant activity limitations and health-related quality of life (HRQoL) below population norms (Hodgson et al., 2017). The consequences of PICS on patient and family quality of life, social interaction, return to work, and mental well-being are all encompassing (Yuan et al., 2021).
How best to support survivors through the myriad of issues post-ICU is a growing concern. There are several studies and meta-analyses exploring recovery interventions for ICU survivors. Formal follow-up clinic settings and nurse-led phone follow-up are most often described (Haines et al., 2019; Jensen et al., 2015; Leggett et al., 2024; McPeake et al., 2019; Schofield-Robinson et al., 2018). Early models using a formal post-ICU follow-up service in the United Kingdom (UK) and the United States were created over two decades ago and are now considered a standard of care (Nakanishi et al., 2024). This model consists of a nurse-led, multidisciplinary team approach to providing information, assessment of needs, and psychological support to patients and their families in a hospital setting (Lasiter et al., 2016; Nakanishi et al., 2024). Other more recent models, such as peer support and telehealth/virtual follow-up, are starting to emerge (Lasiter et al., 2016).
Currently, in Australia, ICU follow-up services are limited, and care of survivors is provided almost exclusively by their primary healthcare practitioners (such as general practitioners and nurse practitioners) (Cook et al., 2020). Anecdotally, this is also the case in Aotearoa New Zealand. Unfortunately, primary care teams have limited expertise in critical care or ICU survivorship and may not be best placed to provide post-ICU follow-up. To understand what is needed locally, the patient’s lived experience and needs during recovery must be explored in the local context. Currently, there is little to no research exploring PICS, long-term survivorship outcomes, or the recovery experience in post-critical illness in Aotearoa New Zealand (Sutton et al., 2024).
This research describes the experience of critical illness, explores the survivorship journey (from illness onset to six to nine months at home), and issues and needs during that time. Understanding these aspects may provide a platform by which strategies are developed to help support survivors better in Aotearoa New Zealand.
METHODS
Research paradigm, positionality and reflexivity
As first author (LS) I describe here my entry into the research. The constructivist/interpretive approach to this research resonated strongly with me for several reasons. I have extensive clinical ICU experience spanning over two decades working with complex long-stay critically ill patients. This has facilitated a dual perspective as both the gatekeeper of knowledge and the learner of new information, where this work is part of a mixed-methods PhD around survivorship and PICS. My epistemological approach in this research was centred around social constructivism, whereby co-constructing theory collaboratively alongside participants creates a shared understanding of the survivorship experience (Charmaz, 2006). Having had experience following up with participants as part of a cohort study exploring long-term outcomes in an Aotearoa New Zealand cohort (Sutton et al., 2022), I already had some insights into the challenges of critical illness recovery. However, understanding how those difficulties are navigated, including impacts, barriers, and facilitators to recovery, requires a richer analysis that is best done through a qualitative research lens.
The risks of introducing bias and subjectivity, forcing theory, and missing nuances or subtle differences requires careful navigation (Charmaz, 2006). Researcher reflexivity relates to a process of self-awareness, of transparency of inherent bias and assumptions (Charmaz, 2006). Before the interviews began, I assumed that participants would focus primarily on the details of their ICU stay and recovery, as this is my area of expertise. However, it was quickly apparent that participants wanted to tell their story from the start, some describing what life was like before getting ill and the memories of the experiences that led them to becoming sick. Strategies such as careful listening and documentation, field notes, memos, and journalling, stringent line coding by staying close to the participant’s own words were used to ensure participant stories were facilitated but not forced.
Sample and setting
This research is part of a mixed methods design, a protocol of which is reported elsewhere (Sutton et al., 2022). A mixed-methods design was chosen to best explore as many perspectives of recovery as possible within the Aotearoa New Zealand context. A cohort study exploring quantitative measures of PICS and disability at three timepoints in the year following critical illness, started recruiting in January 2022. The qualitative study aimed to illuminate the lived experience of the recovery journey for survivors. Two centres were involved in this grounded theory study, both large tertiary-level ICUs.
A sequential/convenience sampling approach from the primary cohort study (Sutton et al., 2022) was initially used. The inclusion criteria included adult patients (>18 years) in the ICU for 7 days or more or mechanically ventilated for 72 hours or longer. Paediatric, neurosurgical patients, and those who sustained a traumatic brain injury, brain hypoxia, haemorrhage, or neuromuscular disorder were excluded. In total, 22 participants were eligible for the study, 19 were approached, eight declined, and three were lost to follow-up. A total of eleven participants were interviewed. The recruitment period ranged from July 2022 to the final patient in August 2023. After the first five participants were interviewed, purposive sampling was undertaken. This was done to capture a more diverse range of participants. Families were able to be present during interviews to support participants, but their responses were not analysed. Research into the family experience of survivorship is underway elsewhere in Aotearoa New Zealand (Best et al., 2023).
Ethical and cultural considerations
Ethical approval was gained from the New Zealand Ethics Committee (Ethics ID: 21/NTA/107). Consultation with local Iwi from all centres was performed. Before the commencement of the research, there was consultation with the Māori Kaupapa research group, and training through a ‘Tikanga for Researchers’ workshop. To ensure fair representation, every opportunity to recruit Māori participants was taken (including approaching a second centre to help with recruitment). Strategies to prevent loss to follow-up were also diligently undertaken with all participants. Verbal and written consent was gained by all participants before the interviews. A safety escalation plan was developed as part of the study protocol, and participants were informed, they could stop the interview at any time. The safety protocol outlines referral to the participant’s healthcare provider if there is significant distress or a patient safety issue.
Data collection and interviews
The lead author (LS) handled all administrative and data management tasks, including screening, recruitment, consent, data collection, and analysis. Semi-structured interviews, using both open and closed questions, were completed. Ten took place at the participants’ homes, with one in the hospital. Interviews lasted approximately an hour and were conducted in various locations in Aotearoa New Zealand. All interviews were recorded on a university password-protected laptop. Participants received a $50 voucher (koha) after the interview.
Data analysis and coding
Data were analysed initially with meticulous line coding of all transcripts to ensure no details were missed. After each interview, the data were coded and analysed. Codes were organised through several rounds of open, axial, and focussed coding using NVivo11™. Stringent documentation of coding stages, reflections, and theory development was captured in a journal, memos, and field notes. All individual memos and each set of code books were shared at each coding phase.
Each stage of coding and theme development was checked by at least two people, one an expert in grounded theory and the other an experienced academic and researcher. Checking data and developing themes with key project supervisors regularly provided a “second opinion” on the theory-building process and quality control. The end of participant recruitment was determined as the point at which there was enough depth and variation of data collected, and participants interviewed.
Scientific rigour and evaluation criteria
The principles of quality control using the Charmaz Credibility, Originality, Resonance, and Usefulness framework (Charmaz & Thornberg, 2021) were used to guide the quality of the research approach. The Standards for Reporting Qualitative Research checklist (O’Brien et al., 2014) was used to report the methodology and findings.
FINDINGS
Eleven participants were interviewed between August 2022 to July 2023. The first six were in the ICU during COVID-19 visitation restrictions. Participants came from a wide range of demographics, backgrounds, and admitting conditions (Table 1). In total, there were four females and seven males with a mean age of 63 (range 24-75). Participants’ ethnicities included Māori (n=3), Indian (n=1), and New Zealand European (n=7). The mean ICU LOS was 11 days (5-26 days), and the mean hospital LOS was 22 days (7-51 days). This was a complicated cohort, reflective of a longer stay (persistently critically ill) patient group.
Creation of the theory
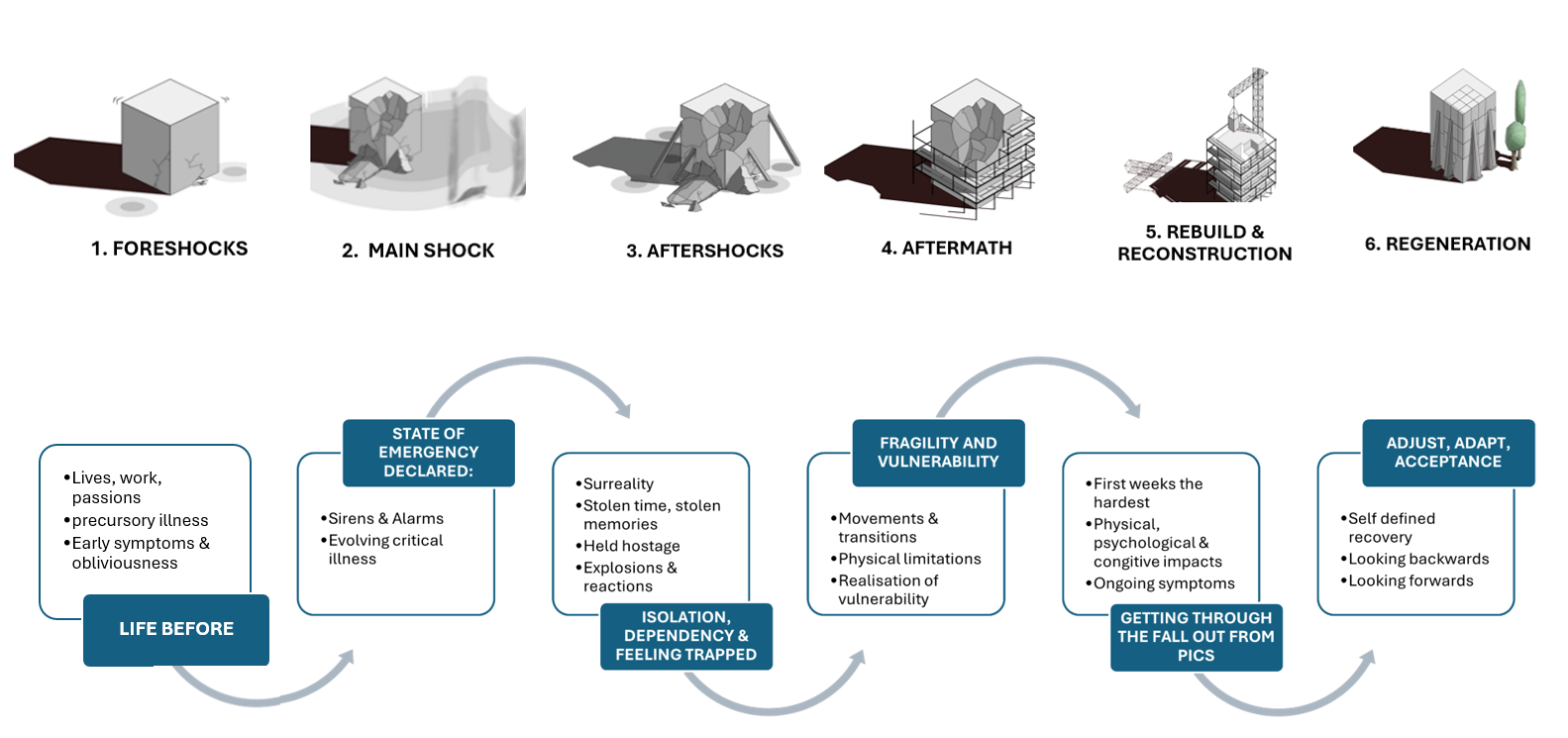
The theoretical concept derived from this study is ‘transitions through the disaster of critical illness’. The survivorship experience analogous to the phases of an earthquake was developed later in the analysis process, after many rounds of coding, discussions, reflections on the data, and overall impressions of all participants’ journeys and experiences. There is a great similarity between survivorship after an earthquake and critical illness (Crowe, 2011). Both experiences can be traumatic and devastating to individuals and communities and can create long-lasting damage that requires time and community support to repair. One participant’s account of critical illness illustrates the concept and analogy overall:
It (critical illness) really shocked and knocked the hell out of me. And you know, I’m a pretty open person, and like to sort of get on with things … but jeez it knocked me back on my heels … you might say like an earthquake … I think the body has had a hell of a shock to the system. It really is trauma based. [P9]
Foreshocks describe the early stages of critical illness, the subtle symptoms that were initially ignored developed as insidiously and unpredictably as the initial minor ‘tremors’ of a developing earthquake (Riga & Balocchi, 2017). As the illness intensifies, symptoms escalate like ‘seismic waves’, as participants realise a disaster is looming. The 'main ‘shock’ describes the full onset of critical illness when ‘emergency response teams’ are deployed. Once in the ICU, patients experience the ‘aftershocks’ of treatment (physical weakness, delirium, surreality, and amnesia). Once in the hospital ward, patients begin to process the ‘aftermath’ of what they have been through. They are fragile and vulnerable both physically and psychologically. It is not until they go home that the extent of PICS is apparent. The early stages of ‘rebuild and reconstruction’ begin. The final stage of ‘regeneration’ requires adjustment, adaptation, and acceptance of ongoing limitations. Like disaster management after an earthquake, none of this is possible without the support of family and community (Crowe, 2011).
The grounded theory model of survivorship consists of six conceptual stages and six core themes:
-
Foreshocks: Life Before
-
Main Shock: A state of emergency declared
-
Aftershocks: Isolation, dependency & feeling trapped
-
Aftermath: Fragility and vulnerability
-
Reconstruction: Getting through the fallout from PICS
-
Regeneration: Adjusting, adapting, and acceptance
A discussion of each conceptual stage, overarching themes, and pertinent subthemes is presented next and illustrated in Figure 1.

TRANSITIONS THROUGH THE DISASTER OF CRITICAL ILLNESS
Foreshocks: Life before
Foreshocks in the context of the survivorship journey are used to describe the preceding events and early experience of critical illness with the theme of “life before”. Participants often reflected on their lives before in terms of their jobs, whānau, and passions in life, and the early signs of illness that heralded a point in time when everything changed. For one elective cardiac participant, the lead-up to his presentation was lengthier, having had a heart attack and waiting on a list for a year until his surgery and ICU admission. All other participants described analogous ‘foreshocks’, such as precursory illnesses, as catalysts for life-threatening decompensation. For example, COVID-19 leading to diabetic ketoacidosis; viral illness progressing to pneumonia; myocardial infarction leading to emergency cardiac surgery, shock, and multiorgan failure; and a blocked coronary graft leading to cardiac arrest and cardiac failure. Symptoms such as vomiting, diarrhoea, weight loss, dyspnoea, and pain were described as common precursors and brushed off with stoicism. Many were oblivious to how serious things were becoming until they found themselves in the ICU:
And then the next day, I said “I’ll come right”, you know, famous last words……..Well, I didn’t come right, and then the next morning I was still crook. [P9]
Commonly, it was family or friends who noticed red flags and alerted emergency services. A transition period, where the family realised how unwell participants were becoming, but participants did not, illustrates the insidious nature of the early-stage critical illness.
Mainshock: A state of emergency
The mainshock of critical illness describes the deterioration at the point when the acute becomes critical, a period heralded by a rapidly evolving critical illness and a point in time where a state of emergency was declared. As the seismic waves of illness progressed and the intensity of symptoms increased, participants realised there was an evolving disaster. This was recounted by severe symptoms and physiological deterioration that could no longer be ignored: legs that did not work, severe vision loss, dyspnoea, and loss of bowel control. This also heralded a psychological shift from minimisation and denial to the sudden realisation of the gravity of the situation. A period whereby the threat to their life and the catastrophe of illness were acknowledged and signalled when families were suddenly gathered around:
It just happened within 24 hours, and I was really short of breath. I knew I was sick my temperature was sky high, and I knew I was really unwell. [P2]
And I remember telling him, “I think I’ve dug my last post” and I know I was really bloody crook so but apparently the rest of the family came I have no recollection. Well, all I wanted to do was say goodbye (visibly upset). [P9]
Aftershocks: Isolation, dependency, and feeling trapped
Once the mainshock of illness had been managed, it was during the “wake-up” period when aftershocks were evident. Delirium and ICU-acquired weakness were commonly experienced, memories imbued with surrealistic images, stolen time, and stolen memories (amnesia). Perceptions of being held hostage, trapped, and caught in explosions and reactions (metaphorically representing the reactions and complications from therapy) were common subthemes described.
When participants talked about memories of the ICU, they all described a highly surreal experience. Nightmares, hallucinations, delusions, and delirium were ubiquitous. The emotional turmoil delirium caused was palpable. Participants described feelings of unease and paranoia, mistrust of healthcare teams, and compelling and highly believable hallucinations and delusions. For example, one participant was convinced people were torturing dogs in the hospital basement (herself an avid dog lover). Another participant described how unsafe she felt at night because of an unpleasant recurring dream exacerbated by being in an isolation room. Further subthemes are described next.
Stolen time and stolen memories
Stolen time and stolen memories described the high levels of amnesia experienced by participants. When participants were asked how much they remembered about their ICU stay, most replied “Not much”. Some participants described not knowing where they were when they woke up and thinking they had died. One recalled being incredulous after his friend told him how long he had been in intensive care as he had almost no memory of these three weeks:
And she [friend] told me where I was and how long I’d been there, and I said, “You’re joking!” she said, “No” and I said, “Are you sure I was here [ICU]?” She said, “Yes, you’ve been out for two and a half weeks” and I was like “What!” [P10]
Trapped and held hostage
A common experience of feeling “held hostage” was prominent in several participant’s accounts. Trapped from the outside world, and isolated from support with visitation restrictions. One participant remembered the sense of isolation from her husband during COVID-19, long into her recovery at home which greatly affected her well-being.
Trapped by dependency and weakness within a dark and imposing environment was also commonly recounted. Trapped in a weak body was described by all but one participant. Physical weakness was hard for participants who valued being independent in their lives before. This relinquished control and dependency on care was difficult. Participants remember wanting to flee and trying to get out of bed to do so:
My son said he would just walk in, and I’d say, “get me out of here”. [P1]
Explosions and Reactions
Explosions and reactions describe the experiences participants had undergoing treatment, and the symptoms, and sequelae from illness and therapies. Participants described emotional responses to the ICU phase, including fear and panic, particularly during desedation, extubation, and liberation from mechanical ventilation. Bowel management was a major source of embarrassment, with common themes of loss of privacy and dignity related to bowel movements. Some felt humiliated by losing bowel control, being placed in nappies, and relying on nurses for basic care. For two participants, the distress and humiliation over diarrhoea persisted long after discharge. Another participant recalled embarrassment, unable to maintain dignity due to physical weakness, compounded by staff entering unannounced:
And people were like, just coming in and I couldn’t move my hands to cover myself. [P8]
Despite, the marked burden of these complications on participants well being, all described how much they valued the compassionate nursing care in the ICU. Terms such as “admired” (the nurses), “going out of their way”, “cheerful”, “well looked after”, “apparent that the nurses meant well”, “kind”, and “fabulous nurses” were used to describe care.
Aftermath: Recognising fragility and vulnerability
Once patients have stabilised, the hospital ward is invariably the next phase in the survivorship journey. Similar issues that affected participants in the ICU continued in the ward. However, this phase was heralded by an increasing awareness of what they had been through. Witnessing other patients’ delirium, ongoing confusion, profound physical weakness, abandonment, feeling vulnerable, and wanting to flee were commonly reported. Many participants had become aware of the precarity of their health and were scared and concerned about contracting a communicable disease like COVID-19 or influenza while on the ward.
The experience of care on the ward was highly variable between participants. Generally, when participants spoke of this period, they recounted feeling very vulnerable and highly dependent on the nurses. Many described feeling less supported, and unprepared for the reduced one-on-one nursing oversight. For some this move was heralded by a sense of feeling ‘turfed out’ prematurely, which was frightening. Even when patients remained in the ICU due to a lack of ward beds and had more time to psychologically prepare for discharge, arriving in the ward still came as a shock:
"But then it [transfer to ward] was a big change. I didn’t realise how different it was going to be. [P10]
Some participants remarked they never saw the nurses, and another worried when medications were late. One participant felt the ward did not understand the high needs of patients recovering from critical illness, especially around physical weakness. This theme of de-escalation of support was especially pronounced during the peak of COVID-19 restrictions for earlier participants but was especially marked for participant two:
And, so, there was absolutely no understanding of the effects of being intubated at all. No help going to the toilet – I remember struggling to the toilet on a walker. And I had to keep stopping, thinking, “I might fall in a minute. I might just sit down.” Because there was no help. There just wasn’t anybody, it was horrendous. [P2]
In contrast, many described the expertise of diligent teams in picking up and managing deterioration. Two participants recounted deterioration on the ward, and the gratitude for the team in providing life-saving interventions:
I think it must have been two or three in the morning when she [ward nurse] picked up the problem, and obviously, she did the right thing, and I’m so grateful for what [happened]. [P5]
In general, the care was pretty good. I mean, it was great. [I was] well looked after. [P4]
Tikanga and taonga
The Māori experience of ICU and hospital care was also captured as a subtheme and there were several examples of tikanga and diligent cultural care during the hospital stay for Māori participants. One participant and his daughter talked about the value and importance of being offered a karakia before cardiac surgery. This whānau further recounted the professionalism of hospital staff in keeping COVID-19 at bay by instituting stringent checkpoints in the hospital. They also described ICU staff going above and beyond, allowing more extended whānau to visit (than would otherwise be allowed) during COVID restrictions. However, it was difficult when wider whānau from elsewhere in Aotearoa New Zealand also wanted to visit but were unable to. One participant’s nephew resorted to sleeping in his car for a week in the hospital car park as he was not allowed in. Another participant described his nephew sneaking into the hospital to be with his uncle, only to be escorted out. For whanaungatanga (family connectivity), all whānau members needed to visit, to see with their own eyes, to keep vigil, and to provide protection. A clear example of this was given by his daughter, who, on visiting her father on the ward, noticed he was ‘not quite right’ and alerted the ward staff. Unfortunately, her concerns were not immediately acted upon, and he subsequently collapsed, requiring resuscitation and transfer back to the ICU. Days later, once recovering on the ward, the participant and whānau describe pride when the doctors and nurses would refer to him as a hero for surviving all his complications. His daughter described him as being precious.
Reconstruction: Getting through the fallout from post-intensive care syndrome
Like reconstructing infrastructure after an earthquake, rebuilding oneself was a slow but necessary process. This generally occurred in a rehabilitation facility or home domicile hospital. Some people spent days in rehabilitation, others spent months. Participants all spoke of their fondness for this time and the compassionate care and time spent talking and connecting with the staff. However, it was the sense of moving forward, becoming less dependent, and the anticipation of going home that fuelled a need to get stronger and improve physically.
Once home
The first weeks were challenging with significant physical limitations, crippling fatigue, and dependency for all but one participant. Functional limitations and loss of physical strength were by far the most common ongoing complication of critical illness, affecting many, for months after. One participant described the dichotomy of both loving and hating her walking aid because whilst it helped her to mobilise, it also symbolised her new dependence and loss of freedom. In contrast, one elective cardiac surgery participant reported his recovery to be very quick, out mowing the lawns the day after discharge. Other common symptoms included balance issues, headaches, pain, dyspnoea, dysphonia, sight loss, taste changes, and skin and hair changes across a range of participants. One quote illustrates how hard it in the early stages:
I wouldn’t wish what I went through in those first two months on anybody. [P1]
Psychological aspects
Emotions such as sadness, loneliness, and frustration were commonly reported. Participants were troubled by their delirium memories and nightmares and thought about them long into recovery. One participant used the term “post-traumatic stress” to describe the experience in the hospital and during recovery. However, mostly it was frustration with slow recovery that was recounted. No participants received psychological support once home.
Cognitive impact
All but one participant reported struggling with cognitive dysfunction during recovery, which was often lingering and persistent. These difficulties largely pertained to short-term memory processing deficits; some participants reported problems with word finding, others not recalling their passwords or how to use once familiar technology and forgetting to take medications.
Regeneration: Adjustment, adaptation, and acceptance
Regeneration after critical illness characterises a period of readjustment, a reflection on what survivors have been through, and a changed outlook on the future. Participants’ recovery was heavily influenced by support from family and friends, who were seen as key to both emotional connection and practical help. One Māori participant felt lucky to have whānau around, which he believed was crucial for his healing despite his prolonged disability. Another participant took a special trip to the coast to reconnect with her whakapapa[1] as a way of healing.
As recovery progressed, listening to their bodies became both a coping and recovery strategy. Participants were mindful of when to rest and, over time, began to rediscover small passions like walking or cooking. Returning to activities like driving and working marked recovery, though regaining these abilities varied. For most, driving took weeks or months due to cognitive issues, slow reaction times, and reduced strength.
Recognising fragility and mortality
Most participants were very conscious of taking better care of themselves to avoid a recurrence of critical illness. One participant relayed feeling scared that her illness was a random occurrence made her feel that it was out of her control, very fearful of ending back in the ICU. When she learned that the cause of her sepsis was not as rare as she had thought, she was relieved. Another participant relayed how the smallest of injuries in the garden could cause her to spiral into panic that she might again develop sepsis.
Unsurprisingly, participants also recognised their mortality through the journey of survivorship. Some spoke flippantly about decluttering the house, downsizing for the sake of finances, selling prized vehicles, and “clearing up”. Mostly, when they spoke of who would be left behind (such as dogs, children, and grandchildren), very little was spoken, but triggered a very emotional response. Some participants recounted only finding out much later how close to death they had been, not cognisant of this until families broke it to them once home. This was very confronting for one participant. Despite all the hardships and challenges, they faced in the hospital, most participants recounted immense gratitude for the care received and skilled dedication of health care staff in saving their lives.
Unfortunately, there was little support from the healthcare system once they left the hospital. One participant found it unbelievable there wasn’t more support or information. Many participants described how they would have liked some follow-up from the “system” to provide reassurance and checking in. Some did not feel the general practitioner was an appropriate person to do this because they did not have expertise in critical care. Getting an appointment was another barrier.
So, ICU was ok. It was the minute I left the doors of the hospital that really let me down. And I do feel quite bitter about that…. It would have been nice to have had support, because I didn’t get anything at the time. It was just me and my husband. [P2]
Moving on
Most participants had re-evaluated their priorities and changed what was important to them. These changes revolved around improving work-life balance, and spending more time on holiday, less time working and making money, and time spent with children and grandchildren are priorities.
When participants reflected on where they were in their recovery, some defined this by the resumption of travel and being able to take a road trip, others by the resolving of fatigue and symptoms and not being so dependent on others. Unfortunately, being ‘not recovered’ was a theme for some participants. Many were positive about the recovery they had made so far but cited ongoing physical and or cognitive issues, headaches, and fatigue. Whilst participants still had hope of further recovery, they also accepted this was generally out of their control.
I’m getting there. Well, you really don’t have a choice. You just got to pull yourself together and get on with it. [P6]
But a lot of people say, “you’re a survivor” and I say “I had to” but it wasn’t easy. [P10]
DISCUSSION
The analogy of critical illness akin to the disaster of an earthquake described in this study is anchored in participant accounts of dependency, complications, and disability that occur during key phases and transitions. The experience of early illness, like the ‘rumbles’ of foreshocks, is unpredictable and insidious until the main shock of illness hits. Aftershocks, synonymous with the complications of ICU treatment, can lead to the functional, cognitive, and psychological sequelae of PICS. This is not unlike the issues disaster victims face after an earthquake (Crowe, 2011). Traumatic memories, delirium, amnesia, pain, grief, loss of independence, and mortality are common antecedents of post-traumatic stress disorder (PTSD), anxiety, and depression (McGiffin et al., 2016). Rebuild after both earthquake and critical illness takes great support from family and close community. In time, there is adaptation and acceptance of a new normal. Lifestyle changes and re-evaluation of life priorities by spending more time with family were key positive changes that participants described.
Whilst the overall earthquake concept is unique to this study, findings are mirrored in other international studies. For example, Kean et al. (2017) and Page et al. (2019) describe the recovery journey also as one of unscheduled passages and movements through transitions and phases. Ultimately, there is a redefinition of self, acceptance of disability, and gaining control of one’s life again. Whilst there are similarities, it was important to explore the survivorship journey within the context of Aotearoa New Zealand; its healthcare system, culture, and people.
One of the notable findings from this study was the relatively negative experience of the hospital journey for some participants. Participants often reported dichotomous and conflicted experiences. On the one hand, many reported compassionate and dedicated nursing care, feeling tightly held in the ICU, and grateful for the team’s expertise in saving their lives. Generally, however, when participants describe the ICU experience, it was dominated by memories of physical limitations, delirium, amnesia, and hallucinations. A systematic review of 15 studies have echoed similar findings, that positive aspects of compassionate care are experienced but are often overshadowed by disability, delirium, fear, and cognitive dysfunction (Maartmann-Moe et al., 2021).
On the ward, participants started to experience the psychological ‘fallout’ from what they had been through when cognitive function and awareness returned. Isolation, lack of care, and feeling abandoned when transitioning from the ICU to the ward were commonly reported. In the ICU, one-on-one nursing ratios have the time and resources to support the care needs of the patient. However, the movement to the ward can be stressful with the changes in resources and oversight, at a time when patients are still highly complex with high psychological support and nursing care needs. This is a universally shared experience commonly reported in the literature (Cuzco et al., 2022; Yumei et al., 2024). For early participants, a perception of lack of care and abandonment was further compounded by a chaotic hospital during the early COVID-19 restrictions.
In Aotearoa New Zealand, the principles of Te Tiriti o Waitangi[2] provides a foundation of care that underpins the health and disability system. The principles include tino rangatiratanga (Māori self-determination and involvement in the design and delivery of health and disability services); equity (equitable access to services and treatment to ensure improved health outcomes for Māori), active protection (actively working to equitable health outcomes for Māori); options (access to kaupapa Māori health and disability services); and partnership (co-designers of the health system for Māori) (Ministry of Health, 2024).
The importance of whakawhanaungatanga (relationships and making connections) was crucial for participants in this study. For example, one participant described compassionate care, feeling included in the rehabilitation team when staff connected over their family stories when he was missing his whānau. For Māori, health as a taonga (precious) involves strong connections with others and is inherent to building a relationship based on trust (Komene et al., 2024).
Whakawhanaungatanga is a crucial aspect of Te Tiriti principles of active protection and participation. It is also a vital aspect of caring for the critically ill patient alongside the family. Facilitating whakawhanaungatanga is a unique opportunity to provide protection, but it is also an opportunity for whānau to be active participants in their loved one’s care, facilitating presence, strengthening trust, engagement, and kōrero (communication) with the health care staff (Komene et al., 2024). For whānau, one way to provide whakawhanaungatanga is through continuous ‘bedside vigil’. For this continuous bedside vigil, one participant recounted great gratitude when ICU staff went out of their way to facilitate more than the usual visitation for one participant.
Unfortunately, not all whānau were allowed to visit and close family found it hard to maintain their role of kaitiaki. This practice also appears to be regionally disparate; some families offered wider visitation, others did not. One example of the power of family protection was highlighted by an account of healthcare staff not listening to the concerns of a participant’s daughter when she noticed subtle deterioration in her father. This led to a return to the ICU for resuscitation after he collapsed. Despite efforts to embed the Te Tiriti principles in health policy and nursing practice, there is a consistently reported lack of engagement and connection from healthcare staff during inpatient care as this example illustrates (Komene et al., 2024). Research over the last two decades has found the hospital experience both hostile and alienating for Māori (Graham & Masters-Awatere, 2020). Not only is there cultural alienation and racism but there is also little relational rapport and ineffective communication and power imbalances (Graham & Masters-Awatere, 2020). Tino rangatiratanga[3] is about trust, power sharing, effective communication, and empowering patients and their whānau to be active participants in their care (Edmonds et al., 2024; Ngata, 2020).
IMPLICATIONS FOR PRACTICE
Facilitating whakawhanaungatanga
Applying the principle of whakawhanaungatanga widely in the ICU for all patients (irrespective of cultural background) is likely to be very beneficial, especially in terms of patient safety, and enhanced care (Bowman & Beesley, 2025). Family participation in care has already been extensively researched internationally (Olding et al., 2016), with a scoping review identifying several key benefits, such as enhanced patient safety, having needs met/being supported, improved communication, shared decision making, and contributing to care (Olding et al., 2016). In order to do this, however, healthcare staff need to be actively engaged and educated in how to facilitate the principle of participation in care and whakawhanaungatanga. Furthermore, open visitation, adequate hui rooms, provision of the basics such as food and hydration, seating, and ‘waiting rooms’ that offer comfort in a culturally safe space is also essential for whanau but often lacking (Masters-Awatere et al., 2024). A local quality improvement project recently rolled out, “Kaitiaki; partners in care,” aims to support patients in hospital with a nominated Kaitiaki (family guardian) (Health New Zealand, 2022).
Transition to the ward
Several key issues are evident from this study which warrant improvement. The transition from the ICU to the ward is fraught with anxiety, unpreparedness, and abandonment. This is reported unequivocally in the literature as a key source of anxiety and stress for patients (Nikolaisen et al., 2023; Page et al., 2019). Strategies to improve transfer to the ward from the ICU must begin with an exploration of local processes with quality improvement initiatives around handover, communication of patient needs, and education of receiving staff.
Aftercare and follow-up
In light of recent government funding aimed at increasing bed capacity and expanding intensive care services in Aotearoa New Zealand (Longmore, 2023), it is equally important to shift focus towards supporting survivors. However, healthcare services continue to suffer from underfunding, often driven by political agendas and the control of the party in office at the time.
At a time when survivors need help and support the most, unfortunately, abandonment from the system, limited support, information, and ongoing care is apparent. Not only do survivors endure persistent disability and poor long-term outcomes, but there is also an increased risk of readmission back to healthcare, increased mortality, increased fall risk, cognitive decline, and inability to return to work (Hodgson et al., 2017, 2018; Wilson et al., 2020). This has implications for healthcare expenditure, individuals and communities, and contribution to the workforce (Su et al., 2025). One way to support survivors through recovery is by a dedicated post-ICU follow-up service (Dimopoulos et al., 2024).
Currently, in Australia and Aotearoa New Zealand, there is limited ICU follow up services. For example, only two units in Australia offer dedicated Intensive Care follow-up clinics (ICFC), of which only one is funded (Cook et al., 2020). One study showed that a nurse-led home or facility visitation within eight weeks of hospital discharge reduced the length of readmission days by approximately six days (Daly et al., 2005). Other studies report benefits in survival, functional status, anxiety, depression, and posttraumatic stress disorder (PTSD) symptoms (Jensen et al., 2015; Rosa et al., 2019). The optimum follow-up timeframe, method, and model remain uncertain. Novel methods of follow up such as peer support groups and digital telehealth are under investigation (Leggett et al., 2024). However, phone follow-up within the first three months of discharge home appears to be a commonly used model (Nakanishi et al., 2024).
The discourse around how best to support survivors continues, but follow-up (by any method) is clearly needed. A second paper from this study exploring how follow-up could be delivered in the New Zealand setting is anticipated to be published in early 2025. A follow-up system that is culturally appropriate and equitable should be at the forefront of a proposed follow-up model. Māori consultation should be at the forefront in the design of this follow-up service. Using a model such as Te Whare Tapa Whā[4] (Durie, 2004) for example, would provide a culturally appropriate lens in which to assess and manage PICS The benefits of using this model may extend beyond Māori, supporting the well-being of all patients through its emphasis on physical, psychological, spiritual, and family health (Rochford, 2004).
Strengths and limitations
Strengths of the study include the depth of exploration of the whole of the survivorship journey using a systematic constructivist grounded theory methodology. However, this is a small study among participants from only two centres in New Zealand and participants were a complex cohort with a longer length of ICU stay. Because less complex (shorter stay) patients were not included in this study, it is unknown how their recovery journey differs from that of the cohort in this study. Caution should be used when generalising to other ICU patient types across other units and centres. We were also not able to capture the family’s voice in this research, which is another limitation. The biggest limitation, however, was the inability to incorporate a Māori researcher and co-design model into this research. Whilst consultation with the Kaupapa Māori research network did happen, having a Māori researcher alongside would have provided a culturally rich perspective, one that is unique to survivorship in Aotearoa New Zealand.
Finally, it is important to acknowledge that this study began at the outbreak of COVID-19 and may have impacted the first six participants’ experience of the hospital journey especially so for the first three, who were admitted at the height of the visitation restrictions. However, when all the participant narratives are compared and contrasted over time, there are tangible similarities among the survivorship experience for all participants.
CONCLUSION
This is the first research of its kind to explore the survivorship journey for critically ill patients in Aotearoa New Zealand. Survivorship is more than just about being alive and getting better. It is a journey through difficult and distinct transitions, where surreal memories of the ICU, and subsequent disability downstream where PICS is experienced. Transitions are inherently frightening and once home, support abandonment from the health care system is evident. An ICU follow-up service structured around addressing the aftermath of critical illness during recovery (especially psychological support post-delirium) would be of huge benefit to survivors. However, this should be delivered in a culturally appropriate way, and within a holistic te ao Māori lens.
Acknowledgements
Dr. Ben Daniel (University of Otago, Dunedin, New Zealand) for his support, teaching, and oversight throughout this research project and the following Waikato nursing research team: Amelia Butler, Kara Trask, and Jessica Newland. Jason Elliot for help with the design of the concept illustration.
Funding
PhD funding was received in 2021 for travel and administration costs for the qualitative study from the following sources: 1) Wellington Medical Research/Research for Life (RFL): $6,490; 2) Perpetual Guardian Nursing fund: $10,000. With gratitude.
Conflicts of Interest
None
Whakapapa is a Māori term meaning ancestry and connection to the land and iwi (tribe)
Aotearoa New Zealand’s founding document, (a partnership between Māori and the British Crown) to align the principles of Rangatiratanga (Māori self-determination), equity, protection and partnership.
Refers to self-determination, sovereignty, autonomy, self-government.
Te Whare Tapa Whā is a Māori model of health and wellbeing depicted as a wharenui/meeting house with four walls. These walls represent taha wairua/spiritual wellbeing, taha hinengaro/mental and emotional wellbeing, taha tinana/physical wellbeing and taha whānau/family and social wellbeing. The connection with the whenua/land forms the foundation.