
INTRODUCTION
Nurse educators in the tertiary sector hold substantial responsibility in preparing tomorrow’s nurses to shape the future of healthcare. The nurse educator’s role should be highly desirable in recognition of this contribution – so why is it not? In Aotearoa New Zealand (Aotearoa) and globally, nurses are not choosing careers as nurse educators. The World Health Organization’s (WHO) (2020) State of the world’s nursing report, identified one of the biggest challenges in nurse education is the recruitment and retention of sufficient numbers of qualified nurse faculty. The latest full workforce report from the Nursing Council of New Zealand (NCNZ) (2023b) lists a very small proportion (2.9%) of registered nurses (n = 1858) who practice in nursing education. A recent scoping review (Tower et al., 2024) identified key factors that influenced academic intentions to stay or leave nursing or midwifery education practice. Retaining nurses in education practice required attention to promoting positive work environments through teamwork, building professional relationships, and offering professional development opportunities. Reasons for leaving education practice were linked to emotional exhaustion and burnout and a lack of recognition and valuing of their roles (Tower et al., 2024).
The role of the nurse educator in the tertiary education setting is complex as it straddles both a practice discipline and an academic discipline. Educators in the tertiary sector become dual professionals: they have expertise in a discipline area; and they are teachers (Suddaby, 2019). A successful nurse educator is expected to be an expert practitioner, a skilled educator, and involved in research knowledge generation or translation (Pool, 2021). As the landscapes of practice have become more complex and varied, the nurse educator needs a range of knowledges and actions to match the practice environment (Doane & Brown, 2011). Being able to teach and becoming an academic engaged in research and higher learning may not necessarily be a part of a nurse’s previous experience and, therefore, there are fewer transferrable skills and knowledge to carry over into the role of the nurse educator. The NCNZ (2024) education standards for undergraduate nursing programmes match the WHO (2016) global requirements that nurse educators have a postgraduate qualification, preferably a master’s degree, as well as a teaching qualification. These requirements suggest that experience in higher education and teaching is also valued in nursing education.
However, it is unclear how this combination of clinical practice experience, a postgraduate qualification and a teaching qualification enable or support the formation of the nurse educator. Professional identity development in higher education is described as a way of being and a lens for evaluating, learning and making sense of practice (Trede et al., 2012). Identity can be viewed as the way a person is both similar to and different from others. As professionals, identification includes similarities in knowledge, skills, values and ways of being that are shared by members of the profession. Even with these similarities, further differences can emerge that result in the formation of one’s own professional identity/ies (Lawler, 2008).
Drawing from a wider doctoral study that examined the everyday work of the nurse educator (Pool, 2021), this article argues a need to understand identity formation to recruit and retain a more culturally and gender diverse nurse educator workforce in Aotearoa to better reflect the nursing students and communities served. The formation of the nurse educator can be understood as a “process of becoming: a time of formation and transformation, of scrutiny into what one is doing, and who one can become” (Britzman, 2003, p. 31). The notion of becoming helps in understanding that identity formation can change or reinforce what is learned as well as changing or reinforcing the habitus of the person. “In this way, a person is constantly learning through becoming and becoming through learning” (Hodkinson et al., 2008, p. 41). This article presents a strategic vision for agentic identify formation of the nurse educator in Aotearoa that is enabled through an understanding of cultural and gender biases inherent in the field of nursing education. Adopting this vision may support the growth of gender and culturally diverse nurse educator workforces both in Aotearoa and in other countries also seeking to address equity.
RESEARCH APPROACH
The aim of this doctoral research was to investigate the work of the nurse educator in supporting the professional formation of nurses within the social world of nursing education. For the purposes of the study, a nurse educator was defined as a registered nurse who teaches on an undergraduate bachelor’s degree nursing programme in a tertiary institution. Undergraduate nursing education in Aotearoa New Zealand involves three years of full-time study in a tertiary institution, either at a polytechnic or university, to complete a Bachelor of Nursing (BN) degree.
I undertook this research as an insider researcher who identifies as a white settler (Pākehā) having spent most of my nursing career in nursing education in Aotearoa. I have been privileged to work in an environment with a rich cultural history with values informed by an authentic partnership with local iwi based on Te Tiriti o Waitangi (the Treaty of Waitangi) principles. These values and experiences informed the theoretical framework that underpinned the research study. Drawing on the work of Smith (1987, 1992, 1999), a Canadian feminist sociologist, this research adopted a feminist standpoint approach to account for the complexities of multiple, competing, fluid and intersecting gendered and cultural identities in nursing education practice.
Adopting a women’s standpoint, this research problematises nurse educators’ diverse situations as mainly female academics, while attending to the gendered institutions of nursing and education, and the material and historical structures that frame this work. Bourdieu’s concepts of capital, agency, field and habitus (Power, 1999) were used to examine text-mediated relationships and power. The value of Bourdieu’s theoretical perspective is in the acknowledgement of the range of agency that is constrained or enabled by factors related to status, gender, ethnicity, discipline or institution (Gonzales, 2014).
It is worth noting that this research did not follow the normative structuring of a conventional nursing research thesis, which mimics the theoretical principles and checklists of scientific practices (Grant, 2016). The reader may therefore be confronted by what is presented, and what is absent, in what follows. A qualitative research process provided a familiar pattern for this research that is situated across science and social science research paradigms. The blurring of the line between data collection and data analysis, including the perception of literature review work as data and research in its own right (Smith, 1999), aligns with a postmodern approach including a leaning towards post-qualitative research. According to St. Pierre (2019), post-qualitative research is not a methodology but is an approach that is invented and created differently each time. Metaphors used for such bi-modal research include to look through two lenses or to walk in two worlds to illustrate the complex aspects of practice in new ways (Richardson & St. Pierre, 2018).
Familiar scientific terminology and structures such as data collection and analysis are used without being bound to the conventions of a scientific qualitative research approach. For example, a review of the literature is an expectation in qualitative research in both justifying the reason for a research topic and for providing an understanding of and context for this research topic. For this research, the literature forms part of the textual data to read and make meaning.
Semi-structured interview data
Data collection included interviewing experienced nurse educators working in undergraduate nursing education programmes. The interviews followed a semi-structured format that allowed a conversational style of dialogue while still addressing the interview questions. The interviews provided an opportunity for the participants to share their stories and to explore different aspects of their work.
Formal ethics approval was obtained from the Auckland University of Technology Ethics Committee (AUTEC, Ref 18/253). Ethical considerations included ensuring that participation was voluntary, and that privacy and confidentiality was maintained. I did not interview anyone from my own workplace, but given the smallness of the nursing education community, it was inevitable that some interview participants were known to me. By creating fictionalised narratives based on the interview data, I aimed to maintain the anonymity of participants and their workplaces.
Participants were recruited through emails distributed by nursing education networks with 15 participants from seven different tertiary education institutions (polytechnics and universities) volunteering to be part of this research. Interviews were conducted either face-to-face or on Zoom. The participants interviewed had a wide range of experience in nursing education. Most participants described their move into nursing education as unplanned. Participants spoke of how “an opportunity arose,” or of “sliding into nursing education,” or making a gradual move, starting as a clinical lecturer/teacher then later moving into an academic role. It seemed like a natural progression for some participants to take their clinical experience into the classroom. Because this career move was often unplanned, it meant that participants may not have had a good understanding of what the move meant in terms of the work of a nurse educator.
At the time of interview, some participants were very new to the role (from four to 18 months) while others had been working for 25 or more years in nursing education. The participants’ roles were varied, with job titles including nurse lecturer, senior nurse lecturer, principal lecturer, course leader, acting head of school, programme manager, professional teaching fellow, clinical lecturer, module coordinator and course coordinator. Some participants defined their role more specifically based on their discipline or teaching area; for example, teaching science, simulation lead, Year One BN teaching, or clinical teaching.
Fictionalised and autoethnographic narratives
Writing narratives as a method of data collection and analysis (Richardson & St. Pierre, 2018) transpired in response to the theoretical direction for this research. Texts and mediation of texts were fundamental in forming and creating meanings (Smith, 1992). Data gathered from the interviews and the critical review of literature was interpreted into fictionalised narratives that present the complexity of the social world of nursing education. Text-mediated social relations such as power, and relations of ruling became objects of action or investigation within the text (Smith, 1992). As an insider-researcher, I also mined my own practice in both nursing and education for data through critically reflecting on my experiences as a learner, nurse, teacher, and researcher/academic.
Textual analysis of the interviews was an iterative process of listening to the digital recordings, reading the transcripts, reviewing relevant documents and literature, and writing on-going reflective notes. As part of this creative analytic process, as the researcher I needed to consider how the authors of the stories positioned themselves as the knowers and tellers of the stories (Richardson & St. Pierre, 2018). Through listening and reading for meaning, the social relations were able to be detected by reflecting on how participants understood and differentiated their work as nurse educators. Further analysis looked for those moments in the participants’ discussions that linked to texts or concepts which were rooted elsewhere - outside of their direct experience - but that linked in some way to their everyday work. This process blurs the boundaries between data collection and data analysis.
FINDINGS
Table 1 describes the research narratives written as findings. This article presents extracts from the literature as textual data followed by a creative writing piece drawn from the findings that imagines an ideal nurse educator as an avatar – Te Kaiako Tapuhi (Table 2 and Figure 1). Bourdieu’s concept of habitus is used as a way of understanding identity formation (Hodkinson et al., 2008). Habitus recognises the regularities in behaviour that are associated with social structures, such as class, gender and ethnicity (Power, 1999). Personal values, attitudes, and perceptions shape an individual’s habitus. Through socialisation, an individual’s habitus will mirror the social divisions within their own culture and other cultural contexts (Houston, 2002). These divisions may be linked to education, gender relations and social class. How an individual struggles or makes their way through different social divisions influences the forming of one’s habitus (Gonzales, 2014).
Literature as textual data
The global dominant and normative identity of nurse is portrayed and positioned as gendered female with a cultural identity formed by Western European attributes, values and language (Pool, 2021). The way nurses dress and speak, their titles, their roles, and images of nursing are generalised based on these stereotyped dominant ‘brands’ in the marketplace of identity. Both dominance and subordination are associated with these images alongside privilege and oppression (Pool, 2021).
The Aotearoa New Zealand archetype of the nurse and nurse educator are strongly influenced by the history of colonisation. Inequity and oppression of Māori in Aotearoa can be linked to colonisation and a failure to uphold the principles of Te Tiriti o Waitangi (Chalmers, 2020; Wilson et al., 2022). Te Tiriti o Waitangi is recognised as a relational agreement between Māori and the Crown that guarantees, for Māori, tino rangatiratanga or self-determination or sovereignty (NCNZ, 2023a). Colonisation across health and education systems has not only breached Te Tiriti principles but has contributed to inequities, racism and bias that have privileged the dominant Western Eurocentric culture. The impact of this ongoing dominance, termed as “colonial active resistance to change” perpetuates the existence of racism and ongoing breaches of Indigenous rights (Wiapo et al., 2024, p. 2941). This resistance to change has hindered any meaningful change in nursing education and practice.
The history and cultural practices of Indigenous Māori nurses are not evident in the nurse educator archetype, further marginalising Indigenous leadership and cultural worldviews. This may explain or contribute to the cultural bias evident in the Aotearoa nurse educator workforce with most nursing educators being predominantly older New Zealand European/Pākehā females, with 59% aged 50 years or older (NCNZ, 2023a). A small number of these nurse educators (9.5%) identify as Indigenous Māori (n = 176) (NCNZ, 2023b).
Nearly 90% of the nursing workforce in Aotearoa are female (NCNZ, 2023a). Gender bias is historically attributed to patriarchy structures in both health and education that favour male-led initiatives and disciplines (Apesoa-Varano, 2007; Pool, 2021). Smith (1996) links this positioning in education to knowledge work with women perceived to better suited for roles of knowledge translators through teaching and learning practices. The impact of gender bias for women in nursing education means there are fewer opportunities for leadership due to the constraints of an invisible glass ceiling (Newman et al., 2019). A study of leadership barriers and facilitators in nursing described not only a glass ceiling for women, but also a glass elevator for men, who hold a disproportionately high number of senior nursing roles (Newman et al., 2019). The glass ceiling for women represents the invisible barrier that inhibits women from progressing into leadership positions. Conversely, for men in nursing, their ability to progress is supported by an invisible glass elevator that propels them up the ranks with more speed.
Gender bias has contributed to pay equity issues which were identified as recent deterrents for choosing a career in nursing education (McKenna & Thompson, 2024; Richards & Kieffer, 2023; Salvucci & Lawless, 2016). In Aotearoa pay equity has been an ongoing gender related issue for the nursing workforce with the history of lower pay for women across a range of employment and career spaces including nursing (O’Connor & Alexander, 2020). However, while some advances have been made to address this issue for nurses working in clinical settings, ongoing undervaluing of nurse educators in the tertiary sector has resulted in them earning significantly less than their colleagues in clinical settings (Longmore, 2023).
Addressing the impact of racism, cultural and gender biases is also a global issue that needs attention and voice. Tower et al. (2024) noted a lack of research related to the Indigenous educator workforce. The WHO (2020) report was found to be all but silent in relation to building Indigenous nursing workforces (Chalmers, 2020). Colonial based structures and practices continue to privilege groups of non-Indigenous and white people (Wiapo et al., 2024).
The small number of Indigenous nurse educators in Aotearoa may find no familiarity or comfort in the images of nursing that reinforce the domination of one cultural worldview. In Aotearoa, Indigenous nurse leaders also face the ominous task of seeking actions to address inequities for Māori that have resulted from constraints in the health workforce and healthcare systems that are culturally biased towards the dominant culture of Pākehā New Zealanders (Wilson et al., 2022). Steps have been taken to grow a culturally diverse workforce through the development of Indigenous nursing programmes led by Indigenous nurse educators and leaders (Mullane et al., 2023). However, increasing the numbers of Indigenous nurses alone fails to address the compounding issues of racism and the inequities experienced by Indigenous nurses (Chalmers, 2020; Wiapo et al., 2024). Indigenous ways of knowing need to be given priority over the goal of diversity in the workforce (Chalmers, 2020; Wilson et al., 2022) to support the shift of agency and power in the field of nursing education. A strategic vision to support authentic identity formation that might address cultural and gendered bias are proposed by visioning an avatar that draws on Māori wisdom to embody the ideal nurse educator.
Creating Te Kaiako Tapuhi
Earlier narratives in this research invoked an archetype for describing historical or usual practice of the nurse educator. The avatar is a future-facing embodiment of a person which may be new, unexpected or revolutionary (Merriam-Webster, 2021). In the digital world, a person can choose or create an electronic embodiment. The identity formation of the agentic nurse educator might be thought of as somewhat analogous to creating an avatar.
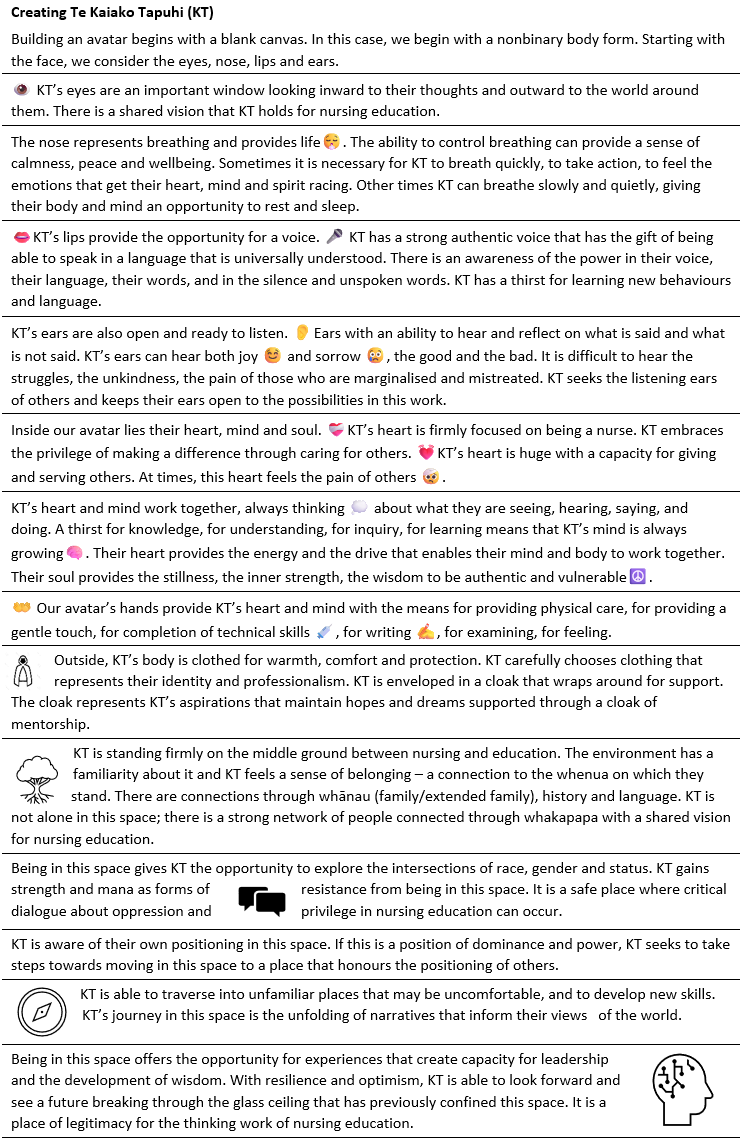
Table 2 is the creative narrative that describes the avatar, Te Kaiako Tapuhi that is envisioned from the research findings. An artist’s impression of Te Kaiako Tapuhi based on this creative narrative is included as Figure 1. Kaiako is a Māori word meaning teacher/educator and tapuhi is a Māori word meaning nurse that is used adjectivally and hence following the noun – educator - in this phrase, according to the syntax of te reo Māori (the Māori language). The use of te reo to name this avatar signifies the cultural capital from a te ao Māori worldview, as part of an intention towards normalising te reo Māori within the process of envisioning an ideal nurse educator in Aotearoa. Te Kaiako Tapuhi, the avatar, represents the identity or habitus of the Aotearoa undergraduate nurse educator, with some of the unique characteristics, attributes and experiences of the local context. The value of viewing nurse educators as somewhat like an avatar in an electronic medium is their inherent ability to change and be modified and enhanced as it grows and experiences different opportunities in the changing fields that it may encounter. I use the term kaiako tapuhi to mean the nurse eductor (or nurse educators) of the future as they draw from Te Kaiako Tapuhi to guide their identity and practice.
.png)
Building an avatar begins with a blank canvas. In this case, we begin with a nonbinary body form. Starting with the face, we consider the eyes, nose, lips and ears.

DISCUSSION
The vision of Te Kaiako Tapuhi as the ideal nurse educator offers a strategic vision to support authentic identity formation of kaiako tapuhi (nurse educator/s). Te Kaiako Tapuhi, as an avatar, embodies authentic identity and voice, not being described in an objective binary of either authentic or inauthentic. Rather, for kaiako tapuhi, an authentic identity will develop over time as they change and develop their own authentic self. Te Kaiako Tapuhi can be conceptualised as an agent with unfolding narratives that inform their views of the world and guide actions taken to navigate within their role as kaiako tapuhi.
The struggles kaiako tapuhi may experience in their identity formation contributes to their vulnerability. Authenticity and vulnerability are viewed as critical in forming trusting relationships especially for Indigenous nurse leaders (Wiapo & Clark, 2022). Indigenous concepts of leadership do not hide vulnerabilities (Wiapo & Clark, 2022). Being vulnerable in a relationship results in sharing the authenticity of what it is to be human. The vulnerability that the new kaiako tapuhi experiences is in developing authenticity as a teacher and academic. Sharing this vulnerability in relationships with learners and colleagues enables kaiako tapuhi to develop an authentic voice in a variety of contexts. Critical thinking, ongoing professional development and learning, scholarly activities and research all contribute to the development of an authentic kaiako tapuhi voice. Vulnerability is a necessary part of this journey, not something that should be avoided or hidden; rather, it should be embraced.
Listening respectfully and openly embracing vulnerability, authenticity and unknowing is described as a process of cultural humility (Fraser, 2022). To be authentic, a person needs to seek to know their authentic self by situating themselves in the unknowingness of being other (Porr, 2005). Fraser (2022) challenges nurses to “bear witness” (p. 4) to the truths of colonisation through listening to the stories of others with kindness and compassion in a relationally accountable manner. Kaiako tapuhi need to be able to dialogue about practice in a manner that honours the knowing of the other with a self-awareness of the authority and privileging of dominant worldviews. To develop authenticity as kaiako tapuhi, the impact of gender and cultural bias on knowing the other must be understood.
The findings from this research were missing any substantive dialogue that addresses experiences of gender and cultural bias. The silence or unspoken acceptance of these biases in nursing education is not unexpected. The lack of voice regarding these issues signals the absence of resistant and linguistic capital to address these issues. The research report commissioned by the Nursing Now campaign recognised gender discrimination, bias and stereotyping inhibit opportunities for female nurses as leaders and as decision makers (Newman et al., 2019).
Te Kaiako Tapuhi, as an avatar, encourages kaiako tapuhi to address issues of power, equity and culturally safe practice to reflect the diversity of Aotearoa and recognise Māori as tangata whenua (the Indigenous people of the land). An understanding is needed of the societal norms that have resulted from the discourses that connect kaiako tapuhi identity and attributes to gender and culture. A feminist standpoint approach is needed to understand the impact of gender and culture on kaiako tapuhi identity.
Intersectionality was first adopted as a feminist approach focused on understanding the effects of race, class and gender on women’s identity, experiences and struggles with power (Davis, 2008). It has value both in understanding individual experiences of identity formation as well as in examining intersections of social structures and cultural discourses. Exploring the intersections of race, gender, and status is critical for examining issues of justice and equity for those who are marginalised (Pauly et al., 2009). It prompts policymakers and researchers to think beyond gender and culture to look at broader social forces such colonisation and oppression (Chalmers, 2020; Clow et al., 2009; Wiapo et al., 2024).
An intersectionality approach begins with examining how people identity themselves, how they are seen with others and how they interact with others. For many nurse educators, this requires personal reflection on the privilege of being white and middle class and recognising the struggle for minority populations who are marginalised and oppressed. Part of the challenge of this reflection is understanding how one’s own identity contributes to these normative discourses (Van Herk et al., 2011). Processes of norm awareness and norm criticism may help to deconstruct, destabilise, and question dominant societal norms by scrutinising the power structures that create unequal relationships (Tengelin et al., 2020). Thinking about how gender pronouns are used and other language biases that privilege or oppress are simple approaches to deconstructing and creating a more authentic identity for kaiako tapuhi.
Social location or the amount of privilege and oppression that an individual possesses on the basis of their specific identity must also be considered as an integral part of an intersectionality framework (Hulko, 2009). Nurse educators who are socially located in positions of privilege due to different educational opportunities and socio-economic factors, and those who come from a position of oppression due to the impact of racism, colonisation and institutional racism will experience their identity differently. Intersectionality attempts to account for the overlapping and interrelated aspects of an individual’s identity and their social location that is influenced by historical relationships and power (Hulko, 2009).
Nursing education provides a powerful socialisation experience in the identity formation of the nurses of the future, shaping both who will be nurses and how they will nurse (Van Herk et al., 2011). The voices of nurse educators need to be shared and heard without the gendered portrayal that has created expectations, structures or actions based on the stereotyped attributes of a dominant or marginalised gender. Introducing the ideal of Te Kaiako Tapuhi, as represented in the avatar, is needed to critically dialogue about oppression and privilege in nursing education and the impacts that it has on the profession, on nursing practice and on health outcomes. An intersectionality paradigm can also be used to appraise and create more inclusive and equitable policies and structures in nursing education (Van Herk et al., 2011).
The work of the nurse educator is viewed from a position of privilege. Future kaiako tapuhi need to reflect the diversity and culture of society. Kaiako tapuhi need to lead by example, as they play a significant role in the formation of a nursing workforce that is able to address issues of social justice and equity. Gender-transformative and culturally safe education is needed in education and health policies and programmes in a manner that positively promotes the position of women and other gendered or culturally marginalised groups (Newman et al., 2019). Kaiako tapuhi need to develop an authentic way of being in the field of nursing education that embraces approaches to actively address inequity. Approaches need to include communication and use language in a manner that supports diversity, inclusiveness, and equity. Leadership and wisdom are needed. Indigenous people who have often experienced inequity and oppression should be supported as leaders who can offer an authentic voice to this discourse.
These research results must be understood as coming from the dominant cultural perspective. The possibility of social exclusion due to strong over-bonding among nursing staff positioned in a dominant culture must be recognised and addressed. A whānau-centred approach is proposed to create and support connections in an inclusive manner that is respectful of diversity. The outcomes of positive, inclusive social networks in the workplace include healthy behaviours and higher job satisfaction (Xu et al., 2020). Other benefits include the retention of staff, and improvements in organisational and professional outcomes through knowledge sharing. The benefits arising from positive collegial environments can extend beyond the workplace to yield better quality outcomes for patients and communities (Xu et al., 2020). Fulfilling career pathways for kaiako tapuhi can be built based on aspirational mentorship offered in a supported workplace environment.
Kaiako tapuhi need collective leadership and voice to thrive in an academic career that offers more than economic reward or status. Yet most nurses are not empowered and do not aspire to leadership positions as they navigate the intersections of motherhood, ethnicity and gender (Aspinall et al., 2021). The global Nursing Now leadership report (Newman et al., 2019) identified that female nurse leadership is hampered by significant challenges that also impact on leadership in nursing education. The first challenge for female leaders in nursing is the ongoing perception of nursing as a “soft science,” thereby less rigorous and inferior to medicine or other science-based disciplines (Newman et al., 2019). Instead of striving to make nursing education more science-based, authentic nursing education leadership needs to build on the cultural capital of nursing knowledge that embraces both science-focused and relationship-focused practice that will address inequity and disparities in health outcomes. The second significant challenge for female nursing leadership is in regard to the gender stereotypes that favour men in leadership positions and the perceived lower status of nursing as a female-dominated society. The cumulative effect or impact of the intersections of gender and culture continues to privilege white people, mostly men in “climbing the hierarchical ladder” into leadership positions in the health workforce (Aspinall et al., 2023, p. 2478). This is a global challenge, where patriarchy and male dominance in leadership and power is indoctrinated into society (Smith, 1987). The third challenge is in relation to pay parity and pay equity issues. Collective leadership and voice are needed from the whole nursing sector and from the wider health and education sectors to develop strategies that build and value the critical nursing education workforce. Policies that address implicit bias and racism in the workforce are needed (Aspinall et al., 2023; Wiapo et al., 2024).
This research has identified multiple challenges reflecting issues of gender, race, culture, indigeneity. Nursing education needs to embrace the opportunity for developing nursing education scholarship that includes both science-focused and relationship-focused practice. This article seeks to contribute as an example of nursing education scholarship that sits in this space. The creation of an avatar – Te Kaiako Tapuhi – provides an opportunity for nursing to challenge and address the many stereotypes recognised as part of nursing habitus. Authentic leadership is essential to create policies which give voice to those who are in some way marginalised by the dominant societal norms. Nurse educators, as kaiako tapuhi, together need to build self-efficacy that seeks to disrupt the structures and power relations that support the extant culture of nursing education.
These challenges require leaders to engage in risk-taking to consider how best to introduce and implement organisational and educational change (Pardue et al., 2018). A prerequisite for building social capital is developing mutual respect across leaders, the creation and development of social networks to support newcomers, building connections and assisting nurses to reach common goals, and valuing all members (Materne et al., 2017). Kaiako tapuhi in Aotearoa, with a collective voice, have the potential to realise the capital and agency needed to achieve these goals.
CONCLUSION
The avatar of Te Kaiako Tapuhi could be viewed as a fantasy, an ideal or even an impossibility. With all the challenges nurse educators face, it would be reasonable to think that aspiring to Te Kaiako Tapuhi would be challenging to achieve. The significant impact of institutional racism and bias that is embedded in nursing education history, curriculum and practice needs to be addressed with leadership from nurse educators. An authentic workforce with a strong identity and voice that matches the unique and diverse Aotearoa population with capacity and capability to grow the nursing workforce of the future is needed.
The concept of the avatar brings consciousness to the possibility of being a change agent. The characteristics and attributes that Te Kaiako Tapuhi possess are the traits of human beings. There are no magical powers needed to play in the world of nursing education and being authentic and vulnerable is a good starting point. The power of kaiako tapuhi comes from within and from the connections they make in the world. Connections as whānau, firmly situated on common ground and in inclusive language, will go a long way in influencing how we speak, think, act and be as kaiako tapuhi. Collective leadership and voice will give kaiako tapuhi the strength and wisdom needed to realise their full potential in their everyday work. Being kaiako tapuhi will be what nurses aspire to become, with recognition for the value of this work.
This research evokes hope and new beginnings for the next generation of kaiako tapuhi who will develop new ways of thinking and new ways of being. Nursing education history, culture, knowledge and relationships formed through tapuhi and kaiako tapuhi provide the social and cultural capital needed to prepare the workforce for the future. Valuing what nursing education has to offer as academic scholarship will enhance nursing education practice and provide the recognition needed in moving towards a positive career pathway. A collective voice is needed to focus on developing opportunities for both tapuhi and kaiako tapuhi as leaders in their practice.
Funding
None.
Conflicts of interest
None