INTRODUCTION
Every child has the right to the highest attainable standard of health and healthcare services (United Nations Convention on the Rights of the Child [UNCRC], 1989). Governments are obligated to take measures to reduce child mortality and ensure no child is deprived of medical care. While global mortality rates have fallen since 1990, progress has notably slowed since 2015 (World Health Organization [WHO], 2025) and rates remain high, with approximately 6.3 million (age 0-19) in 2023 (United Nations Inter-agency Group for Child Mortality Estimation [UN IGME], 2025). Morbidity is especially high for youth, with leading contributions from mental health disorders, injuries, and sexual and reproductive health issues (WHO, 2024). Changing living conditions, including migration, can decrease morbidity and mortality (e.g., through improved living conditions and healthcare), but also introduce increased health risk (Chang et al., 2022).
Migrant children are at risk of unmet healthcare needs and health problems due to a range of life challenges that impact their health and well-being, such as poverty, language barriers, and limited healthcare accessibility (Chang et al., 2022). A Canadian literature review found that parents’ economic instability, possibly caused by unemployment, may limit their ability to afford healthcare for their children, such as oral care, leading to poor health outcomes (Alshamary et al., 2024). Additionally, language barriers were found to hinder healthcare accessibility, in terms of migrant parents’ ease in scheduling medical appointments for their children (Alshamary et al., 2024). Notably, an array of factors regarding the host country may pose different health challenges for migrants. For example, there may be a less inclusive health system, the cost of medical treatment, and limited capacity to accommodate care for migrants, as noted in Japan (Khin et al., 2025).
Although the impacts of migration on migrant children’s health are well-evidenced (Chang et al., 2022), no universal definition exists (Sironi & Emmanuel, 2019). According to the definition given by the International Migration Organization, migrant refers to an individual who relocates from their place of usual residence for any reason, either temporarily or permanently, within or across an international border (Sironi & Emmanuel, 2019). While the term ‘migrant children’ is rarely defined in the literature, parents’ country of birth was commonly used as a proxy indicating children’s ethnic background (Lin et al., 2014; Park et al., 2024; Wu et al., 2012). For simplicity and clarity, the term ‘Southeast Asian migrant children’ (SAMC) is used in this study to refer to children who were categorised into the following ethnic backgrounds: Bruneian, Cambodian, Indonesian, Laotian (or Lao), Malaysian, Burmese, Filipino, Singaporean, Thai, Timorese, and Vietnamese, or children who have one or both parents originating from countries in the Southeast Asia region. The countries in this region include Brunei Darussalam, Cambodia, Indonesia, Lao People’s Democratic Republic, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam (UN IGME, 2025).
Southeast Asian ethnic groups are categorised as sub-ethnic under Asian ethnicity in national ethnic group classifications, with a significantly growing number now residing in their host country, such as in Aotearoa New Zealand (NZ) (Stats NZ, 2023). However, health information concerning this population, especially children, is often lacking due to this ethnic group being subsumed in aggregated ethnic group data. For example, the health risks of migrant children have been reported within Asian ethnic groups without describing sub-ethnic groups (Argueza et al., 2020). Importantly, evidence indicates discrepancies in health risks or issues reported between SAMC and other sizable Asian groups. For instance, in Taiwan, children with a Southeast Asian background were at higher risk of developmental delays compared to children with a Chinese background (Wu et al., 2012). Disparities in healthcare use between Asian sub-ethnic groups were also noted in New Zealand adolescents (Peiris-John et al., 2022). These findings emphasise the imperative of disaggregating Asian health data and their associated risk factors, which is crucial and necessary to reduce health disparities of this population, especially in NZ (Parackal et al., 2021).
Additionally, factors related to the health needs of SAMC might differ from those of other Asian groups. For example, Southeast Asians have unique traditional health beliefs and practices (Lamb & Phelan, 2008). These characteristics may relate to parents’ health practices and health-seeking behaviours for their children in their host countries. Therefore, the distinctive characteristics of SAMC may identify different health needs from those of other ethnic groups. Disaggregated health studies are crucial for identifying and making visible the hidden health needs of SAMC.
Studies have examined the health needs of migrant children (Argueza et al., 2020; Chang et al., 2022); however, less attention has been given to SAMC, despite their potential risk of adverse health outcomes in their host country. This study provides the foundational knowledge regarding the health needs of SAMC in host countries, which may benefit host countries with limited information on SAMC’s health, such as Aotearoa New Zealand. Presenting this aspect from a broader ethnic perspective has the potential to offer a more comprehensive understanding of how regional dynamics of similarity and difference influence migrant children’s health needs in their host country. Additionally, these findings are essential for nurses, as they provide applicable knowledge for real-world practice to effectively promote the health and well-being of this population.
METHODS
Stage 1: Formulating the review question
A preliminary review identified knowledge gaps and informed the research question: “What are the health needs of Southeast Asian migrant children in their host country?” Health needs in this context are broadly described as health risks or unique strengths related to child health. The inclusion and exclusion criteria are provided in Table 1.
Stage 2: Search and select relevant literature systematically
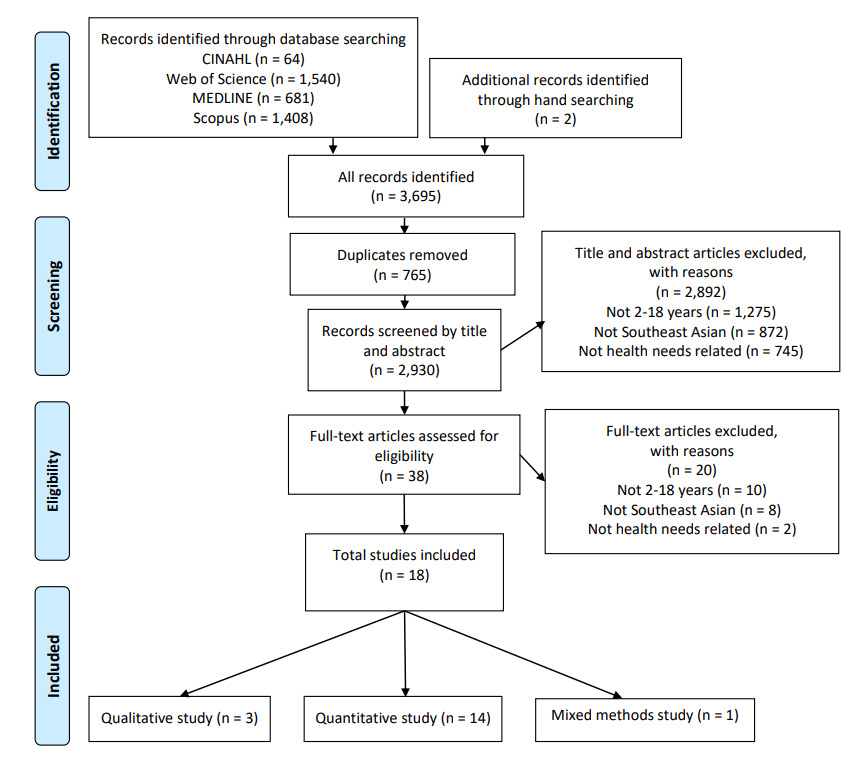
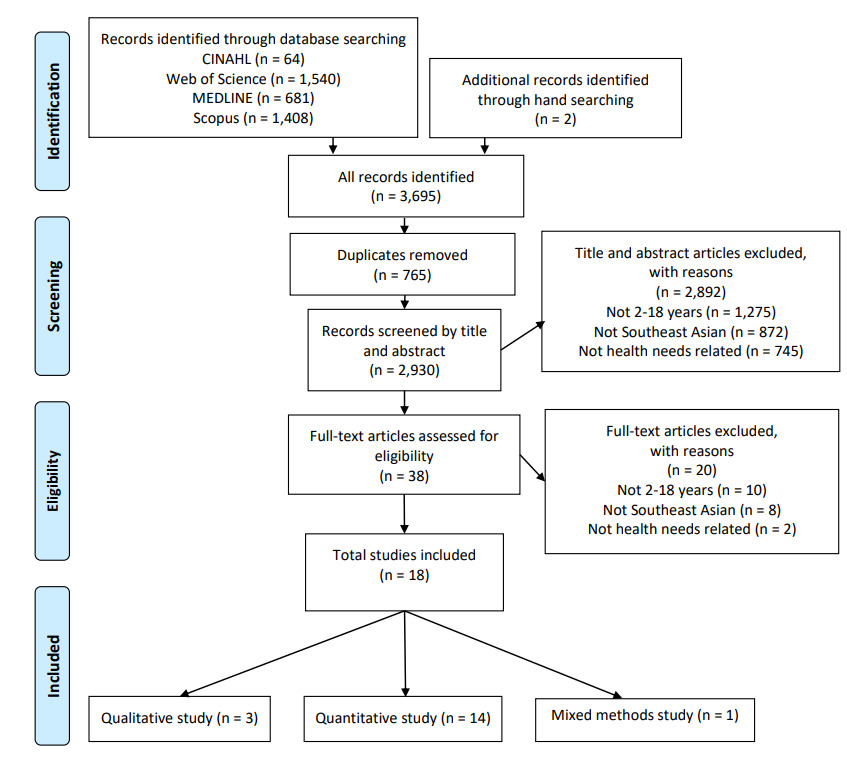
The search was undertaken in early June 2025 using four concepts: health needs, Southeast Asian, migrant, and children. Truncation, Boolean operators (AND/OR), and Medical Subject Headings (MeSH) were used to focus the search (Table 2). Four electronic databases were accessed: Cumulative Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, Scopus, and the Web of Science Core Collection. Hand-searching was used to capture additional relevant literature. A PRISMA flow diagram of the search strategy, based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009), illustrates this process (Figure 1). Title and abstract screening and full-text screening were conducted with the research team. A concordant decision was reached on which studies to include and exclude.
Stage 3: Quality appraisal
This stage was conducted using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018).
Stage 4: Analysis and synthesis
The thematic analysis process, as described by Braun and Clarke (2022), was used to derive topic summaries. Key steps in the process were: 1. Familiarisation with literature through repeated reading and note-taking; 2. Inductive data coding, systematically identifying relevant factors, naming and describing codes; and describing these; and 3. Topic summary generation, collecting related codes into ‘buckets’ and developing descriptions for these groups of codes (Braun & Clarke, 2022). Topic summaries were used due to the heterogeneous nature of the data and limited depth for formal theme development.
Stages 5 and 6: Discussion, conclusion, and dissemination
These stages are provided here.
RESULTS
Of the initial 3,695 citations identified, 38 articles were eligible for full-text screening, and 18 were included (Figure 1). Study quality varied considerably, mostly due to under-reporting (see Supplementary File). The majority were quantitative (n=14; 78%) (Cook et al., 2017; Gleditsch et al., 2024; Guerrero et al., 2015; Guo et al., 2015; Huang et al., 2012; Kjøllesdal et al., 2024; Li et al., 2008; Lin et al., 2014; McKelvey et al., 2002; Park et al., 2024; Tasslimi et al., 2024; Taylor et al., 2012; van Meijeren-van Lunteren et al., 2019; Wu et al., 2012). A summary of the included studies is provided in Table 3.
Six studies focused on physical health issues (34%) (Cook et al., 2017; Guerrero et al., 2015; Kjøllesdal et al., 2024; Li et al., 2008; Lin et al., 2014; van Meijeren-van Lunteren et al., 2019). Another six focused on healthcare utilisation (34%) (Gleditsch et al., 2024; Pham & Vu, 2025; Reece et al., 2009; Tasslimi et al., 2024; Taylor et al., 2012; Vu et al., 2022). Three studies reported mental health issues (17%) (Guo et al., 2015; McKelvey et al., 2002; Park et al., 2024) and one explored child development (5%) (Wu et al., 2012). The remaining studies reported on mixed outcomes (n=2; 10%) (Huang et al., 2012; Lamb & Phelan, 2008).
Across the 18 studies, eight studies (44%) reported results using various broad age ranges, spanning from 2 to 18 years (Guerrero et al., 2015; Kjøllesdal et al., 2024; Lamb & Phelan, 2008; McKelvey et al., 2002; Pham & Vu, 2025; Reece et al., 2009; Taylor et al., 2012; Vu et al., 2022). The other seven studies focused on children of a specific age (39%) (Gleditsch et al., 2024; Guo et al., 2015; Huang et al., 2012; Li et al., 2008; Tasslimi et al., 2024; van Meijeren-van Lunteren et al., 2019; Wu et al., 2012) and with the remaining studies examining children within defined age groups, such as preschoolers, school age children and adolescents (see Table 3).
According to participants’ ethnic background, children with Vietnamese backgrounds were the most frequently included in SAMC studies (n=13) (Cook et al., 2017; Gleditsch et al., 2024; Guerrero et al., 2015; Guo et al., 2015; Huang et al., 2012; Kjøllesdal et al., 2024; Lamb & Phelan, 2008; Lin et al., 2014; McKelvey et al., 2002; Park et al., 2024; Pham & Vu, 2025; Vu et al., 2022; Wu et al., 2012), followed by those from the Philippines (n=7) (Cook et al., 2017; Guerrero et al., 2015; Huang et al., 2012; Park et al., 2024; Reece et al., 2009; Tasslimi et al., 2024; Wu et al., 2012). Brunei Darussalam, Singapore, and Timor-Leste were not explicitly mentioned in any identified studies.
Of the included studies, seven studies (39%) involved children as the sole participants and utilised their health information obtained from databases, health examinations, or their direct responses (Cook et al., 2017; Gleditsch et al., 2024; Guo et al., 2015; Kjøllesdal et al., 2024; Li et al., 2008; Park et al., 2024; Tasslimi et al., 2024). Parents or caregivers were only participants in seven studies (39%) (Guerrero et al., 2015; Lamb & Phelan, 2008; Pham & Vu, 2025; Taylor et al., 2012; van Meijeren-van Lunteren et al., 2019; Vu et al., 2022; Wu et al., 2012). Half of the included studies (50%) were conducted in the United States (Cook et al., 2017; Guerrero et al., 2015; Guo et al., 2015; Huang et al., 2012; Pham & Vu, 2025; Reece et al., 2009; Tasslimi et al., 2024; Taylor et al., 2012; Vu et al., 2022).
Health needs were summarised into four topics: physical health issues, healthcare utilisation, mental health issues, and developmental delays.
Topic one: Physical health issues
Physical health issues were common health needs identified among SAMC. Being overweight or obese and poor oral health were included in this topic.
Being overweight or obese
Being overweight or obese was a frequent health issue noted among SAMC in this review (n=5; 28%) (Cook et al., 2017; Guerrero et al., 2015; Huang et al., 2012; Kjøllesdal et al., 2024; Li et al., 2008). Three studies focused on a specific age (Huang et al., 2012; Li et al., 2008) or an adolescent age group (Cook et al., 2017). The other two reported these health issues across a wider age range, encompassing age groups from two to 11 (Guerrero et al., 2015) and 2-18 years (Kjøllesdal et al., 2024). Three studies focused on this health issue among children from two specific sub-ethnic backgrounds, specifically Filipino (Cook et al., 2017; Guerrero et al., 2015) and Vietnamese (Cook et al., 2017; Guerrero et al., 2015; Kjøllesdal et al., 2024), while two studies reported on Southeast Asian ethnic groups (Huang et al., 2012; Li et al., 2008). Overall, the prevalence of SAMC being overweight or obese ranged from 0.6% to 33%. As three different host countries were included, the prevalence was described separately. The United States was the host country in three studies (Cook et al., 2017; Guerrero et al., 2015; Huang et al., 2012), and SAMC being overweight or obese was reported across various age groups. At age five the prevalence of SAMC being overweight was 13.5% (Huang et al., 2012); with 39.6% of Filipino and 34.1% of Vietnamese children aged 2-11 years found to be overweight or obese (Guerrero et al., 2015); and 26.3% of Filipino and 16.2% of Vietnamese children aged 12-17 years (Cook et al., 2017). Australia was the host country for one study and found 33% of SAMC at age nine were overweight (Li et al., 2008). A Norwegian study reported that 0.6% of Vietnamese children aged 2-18 years were obese (Kjøllesdal et al., 2024). Various factors are suggested as relating to SAMC being overweight or obese. For example, being disadvantaged, such as low family income (Cook et al., 2017; Huang et al., 2012), low parental education (Huang et al., 2012), and high service support utilisation (Huang et al., 2012) were reported. Additionally, parental obesity status and a lack of activity in school were also suggested (Li et al., 2008).
Oral health
Oral health issues were reported in three studies and covered children from four to 14 years (Lamb & Phelan, 2008; Lin et al., 2014; van Meijeren-van Lunteren et al., 2019). Each of these studies reported oral health problems among Indonesian (Lin et al., 2014; van Meijeren-van Lunteren et al., 2019) and Vietnamese children (Lamb & Phelan, 2008; Lin et al., 2014). The prevalence of dental caries among SAMC aged five years in the Netherlands was 16.8% (van Meijeren-van Lunteren et al., 2019), yet 88.7% for those of a similar age in Taiwan (Lin et al., 2014). One study identified oral health-related quality of life as an outcome, reporting that Indonesian children at age nine reported a high quality of life (van Meijeren-van Lunteren et al., 2019).
Contributing factors for dental caries among SAMC were identified as oral health practices and lack of health-seeking behaviours (Lin et al., 2014). Examples of oral health practices leading to problems among 4-6 year-old SAMC included mothers who brushed their teeth less than three times daily, frequent consumption of sugary beverages, not brushing their child’s teeth after consuming sweets, and allowing the child to use the same toothbrush for longer than three months (Lin et al., 2014). Additionally, traditional oral practices among Vietnamese parents and their children, such as delaying the introduction of toothbrushing and using salt as toothpaste, were possibly linked to oral health issues (Lamb & Phelan, 2008).
Concerning health-seeking behaviours, dental services utilisation patterns influencing poor oral health outcomes were identified (Lin et al., 2014). The lack of standard dental visits and check-ups for children aged 4-6 was associated with caries (Lin et al., 2014) and the tendency to seek dental services only when children experience pain (Lamb & Phelan, 2008) may be associated with caries. The latter study also reported that using home remedies, such as salt, to manage oral health issues in children was reported among Vietnamese parents (Lamb & Phelan, 2008). Language barriers were identified by Vietnamese parents as hindering their comprehension of given health information and the scheduling of appointments (Lamb & Phelan, 2008).
Topic two: Healthcare utilisation
Healthcare utilisation of SAMC related to three aspects: vaccination, dental service utilisation and asthma care. Seven studies were categorised into this topic and five of these focused on vaccination (Gleditsch et al., 2024; Pham & Vu, 2025; Tasslimi et al., 2024; Taylor et al., 2012; Vu et al., 2022), with the other two focused on concerning asthma care (Reece et al., 2009) and dental services (Lamb & Phelan, 2008). Two of the vaccination-focused studies reported general vaccine coverage of SAMC at specific ages: two (Gleditsch et al., 2024), three (Tasslimi et al., 2024), and seven years (Tasslimi et al., 2024). The remaining studies focused on issues regarding the human papillomavirus vaccine (HPV vaccine) among children aged 9-18 years (Pham & Vu, 2025; Taylor et al., 2012; Vu et al., 2022). Asthma care was described for children aged 2-10 years (Reece et al., 2009), while dental service utilisation focused on 5-14 year-old children (Lamb & Phelan, 2008). All studies concerning vaccination and dental service utilisation reported on specific sub-ethnic groups, including Cambodian (Taylor et al., 2012), Filipino (Tasslimi et al., 2024), and Vietnamese (Gleditsch et al., 2024; Lamb & Phelan, 2008; Pham & Vu, 2025; Vu et al., 2022). In terms of vaccination coverage, the measles and pertussis vaccine uptake rate among Vietnamese children aged two living in Norway was nearly 100% (Gleditsch et al., 2024). Also good uptake rates were noted among Filipino children in the United States at three and seven years of age for Mumps, Measles, and Rubella (MMR) Vaccine (89.5% and 84.6%), poliovirus vaccine (90% and 84.7%), and Diphtheria, Tetanus, and Acellular Pertussis (DTaP) (80.7% and 83.3%) (Tasslimi et al., 2024). However, the HPV vaccine uptake rates varied considerably, with only 26% of Cambodian children (Taylor et al., 2012) and 63% of Vietnamese children (Vu et al., 2022) receiving any HPV vaccine.
Two key factors contributing to healthcare utilisation for HPV vaccination and asthma care among SAMC were identified: healthcare accessibility and issues related to health information. Economic issues (Reece et al., 2009; Vu et al., 2022), lack of health insurance (Reece et al., 2009), long wait times (Vu et al., 2022), difficulties in appointment making (Vu et al., 2022), and unavailability of primary care providers (Reece et al., 2009) were reported as affecting healthcare accessibility from SAMFs’ perspectives. From the providers’ perspectives, health beliefs, cultural factors, language barriers, and transportation issues were identified as barriers influencing asthma care utilisation for their children among SAMF (Reece et al., 2009). Premigration experiences were reported to influence HPV vaccine uptake among Vietnamese children aged 9-18 (Pham & Vu, 2025). A doctor’s recommendation for vaccination was positively associated with the HPV vaccine uptake rate among Cambodian children aged 9-18 (Taylor et al., 2012; Vu et al., 2022). On the other hand, different languages and medical terminology, lack of translation services, limited knowledge, and receiving inadequate or being overloaded with health information were identified as barriers to Vietnamese mothers’ decision-making regarding HVP vaccination (Vu et al., 2022). However, one study found that health information provided in their native language facilitated understanding; but that reliable health information was typically only provided in English (Pham & Vu, 2025).
Topic three: Mental health issues
Risk of mental health issues was identified among four of the included studies with children aged five to 17 years (Guo et al., 2015; Huang et al., 2012; McKelvey et al., 2002; Park et al., 2024). Two studies reported findings as SAMC (Huang et al., 2012; Park et al., 2024), while the other two focused specifically on Vietnamese children (Guo et al., 2015; McKelvey et al., 2002). One study from the United States reported that SAMC (average age five years) tended to have low interpersonal relationship skills with both high rates of internalising and externalising problems, representing a risk for future mental health issues (Huang et al., 2012). These were explained as the children having low performance in interacting positively with friends, poor self- and emotional control, and exhibiting more negative emotions and lower self-esteem (Huang et al., 2012). Another United States study involving Vietnamese adolescents revealed that exposure to high stress levels in their academic life, as well as friendship and family relationship problems, resulted in high mental health needs (Guo et al., 2015). Bullying was reported among Vietnamese and Filipino 9-12 year-old children in South Korea (Park et al., 2024). This study also suggested that experiencing chronic bullying and victimisation decreased life satisfaction over time (Park et al., 2024). The prevalence of psychological disorders in Vietnamese children aged 9-17 in Australia differed by children’s self-report (15.8%) versus parental reports (4.4%) (McKelvey et al., 2002). In terms of mental health-seeking behaviours, Guo et al. (2015) reported that Vietnamese adolescents were heavily reliant on informal sources for mental health support, including adults (43.3%) and peers (40.2%), with only 4.1% seeking formal support.
Topic four: Developmental delays
Only one study among SAMC indicated the risk of developmental delays, and this was a Taiwanese study exploring child development among SAMC aged three (Wu et al., 2012). The study suggested that these SAMC had lower scores than non-migrant children in three areas of developmental assessment: fine motor skills, language skills, and socio-emotional development (Wu et al., 2012). The study also indicated potential factors relevant to low developmental performance among SAMC, such as a lack of developmental support within their environment, including a limited number of books and limited child-parent interaction (Wu et al., 2012).
DISCUSSION
Overall, this review highlights unmet health needs among SAMC in their host country and that no Aotearoa New Zealand studies were identified. The health needs identified among the SAMC in this review align with the common needs of migrant and refugee children mentioned by the World Health Organisation (WHO, 2021). These findings indicate the importance of adopting a health prevention and promotion approach that considers children’s ethnic context to support their well-being in their host country. Additionally, the health-seeking behaviours described in this review reflect the support of the healthcare system, including access to affordable healthcare, effective health information delivery, and culturally and linguistically appropriate services. Possible explanations for the results of this review are as follows.
Acculturation
Acculturation refers to the process of cultural and psychological changes that occur between two or more cultural groups, resulting in various forms of adaptation (Berry, 2005). These include integration (maintain heritage culture, engage with host culture), assimilation (relinquish heritage culture, adopt host culture), separation (maintain heritage, reject host), and marginalisation (reject both cultures) (Berry, 2005). Acculturation thus encompasses changes in beliefs, values, identity, or behaviours, which can influence the health of minority groups (Fox et al., 2017). Acculturation may be linked to the health needs and health-seeking behaviours of SAMF, including the persistence of traditional oral health practices and a lack of dental visits, mental health concerns, and body weight outcomes.
Regarding oral health, SAMF maintained their heritage oral health practices and showed low uptake of Western oral health practices in their host country. These health practices align with the adoption of a separation acculturation strategy (Berry, 2005), where migrants maintain strong ties to their original culture while rejecting engagement with the host culture. A previous study indicated that separation acculturation in migrant parents was related to the lack of children’s dental visits and suboptimal oral health behaviours (Dahlan et al., 2022), behaviours that were also indicated among SAMF in this review. It is possible that SAMC with low acculturation into the host culture, especially Western culture, tend to rely heavily on their traditional remedies rather than seeking healthcare from formal oral health services and delay in seeking treatment.
Though protective of cultural identity, separation acculturation is also associated with increased anxiety and other mental health challenges in migrants compared with more integrative approaches (Choy et al., 2021). The same systematic review reported that marginalisation acculturation had the worst effects on migrant mental health (Choy et al., 2021). Acculturation is also seen as a barrier to mental health service utilisation among SAMC; however, the dynamics of this relationship remain unclear (Lu et al., 2021). It is possible that separation acculturation impacted mental health and health-seeking behaviours in participants of the included studies in this review.
Acculturation may be partially related to SAMC being overweight or obese. A previous study suggested that acculturation influences eating habits by increasing the frequency of unhealthy food consumption among migrant children who showed stronger preferences for the host culture (Noor et al., 2020), aligning with an assimilation acculturation strategy. However, these findings seem to differ across host country and country of origin contexts (Zhang et al., 2019). In this review, we found considerably different rates of obesity in migrant children between host countries, indicating there may be cultural norms or environmental factors within host countries that impact risk factors for being overweight. Further research is needed in this area.
Overall, culture and acculturation appear to play a crucial role in health needs and health-seeking behaviours among SAMC and their families, impacting health issues found within this population. The need for culturally sensitive healthcare is identified to ensure optimal health outcomes for these communities. However, the variation in the prevalence of these health issues across host countries suggests that other country-specific factors may also be influential, indicating a need for further research to understand the mechanisms of different acculturation strategies on health needs and health-seeking behaviours in SAMC.
Social determinants of health (SDOH)
The social determinants of health are factors related to living conditions that influence health outcomes (WHO, 2023). In this study, low household income, low parental education, and limited health service utilisation were SDOH found among SAMC and the interconnection of these factors and SAMC’s poor health outcomes was noted (Cook et al., 2017; Guerrero et al., 2015; Huang et al., 2012; Li et al., 2008; Lin et al., 2014; Wu et al., 2012). The evidence showed that low household income among migrants hindered their ability to access health services for their children, as some required health services that were unaffordable and were not covered under insurance plans (Salami et al., 2020). On the other hand, migrant children with higher parental education, family income, and insurance coverage had a higher rate of health service utilisation (Dahlan et al., 2022). Education level has been positively associated with health literacy in a systematic review of 156 studies across Asia (Duong & Chang, 2024). This systematic review noted that high health literacy among parents has a positive impact on children’s health outcomes, as health literacy may promote a more conscious approach to disease prevention and treatment (Duong & Chang, 2024). However, in contrast to this review, negative SDOH found among SAMC and their families are suggested as likely to impede their opportunities to receive optimal healthcare, resulting in increased health risks in all domains.
Language barriers
This study found that language barriers were related to how SAMC and their families engaged with healthcare services (Lamb & Phelan, 2008; Reece et al., 2009; Vu et al., 2022). Language barriers hindered the healthcare utilisation process, encompassing scheduling appointments (Lamb & Phelan, 2008), understanding health information (Lamb & Phelan, 2008), and health-related decision-making among SAMF for their children (Vu et al., 2022). A previous study revealed that migrant parents with language barriers struggled communicating with health professionals, such as articulating their children’s health issues and understanding given health information, consequently, restricting their ability to provide appropriate care for their children (Salami et al., 2020). Language barriers also impede SAMF’s health-seeking information in their host country, as health information provided in the host country’s language was found challenging to understand (Pham & Vu, 2025; Vu et al., 2022). Therefore, linguistically appropriate health information is needed to facilitate SAMF’s role in providing care to their children.
Different lenses reflect different health needs
This review highlights the differing perspectives on children’s health from SAMF and SAMC (McKelvey et al., 2002). The prevalence of psychological disorders was higher in children’s self-reports compared to parents’ reports. This finding indicates that children perceived their health issues differently from adults, as can be explained through the sociology of childhood theory (Prout & James, 2015). To precisely understand the health needs of SAMC, a child-centred approach may be the most appropriate way to gain direct input from the perspectives of migrant children, who are typically underrepresented in health research (Smith et al., 2021). Doing so may foster care that is responsive to the specific needs of SAMC, thereby enhancing their health outcomes.
Strengths and limitations
This review explores the health needs of SAMC, a group whose health needs are often subsumed under those of the larger Asian community. By making these needs more visible, researchers can be provided with direction for future research, while healthcare providers can enhance their practice to better serve SAMC. However, some limitations need to be considered. A paucity of literature in this area was noted; therefore, this review may not comprehensively capture the health needs of SAMC. Some sub-ethnic groups, such as Vietnamese and Filipino dominated, which limits generalisation to the larger Southeast Asian ethnic group. Additionally, this review only included published academic literature written in English; future research should include articles in other languages and grey literature.
Conclusions and Recommendations
Southeast Asian migrant children experience various unmet health needs in their host country. Understanding these needs is crucial for nurses, particularly paediatric nurses, to effectively support the health and well-being of children. These findings provide practical insights into health-related issues affecting SAMC, enabling nurses to design appropriate care strategies. The distinction between health needs and health-seeking behaviours reported in this study may facilitate nurses to improve their practice. For example, to address health needs, nurses may adopt a health education approach, aiming to enhance knowledge and promote health awareness targeted at the personal level. At the same time, findings regarding health-seeking behaviours may facilitate applicability by informing system-level improvements. For example, nurses can adopt a linguistically sensitive approach by offering health information in languages used in the Southeast Asia region. From a research standpoint, the health needs and health-seeking behaviours reported in this review may inform the direction of future research to gain a deeper understanding of each health-related variable and the relationships between them, which may provide novel knowledge for improving health outcomes among SAMC.
Funding statement
This work was undertaken by the first author as part of doctoral study, which was supported by a scholarship from the Prince of Songkla University.
Conflicts of interest
None